
|
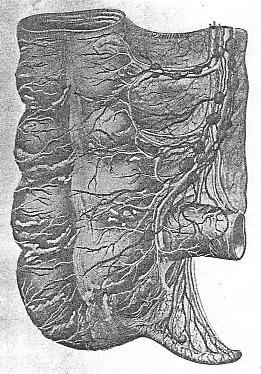
Lymphatics of the Diaphragm While there is a free anastomosis between the plexuses of lymph vessels on the thoracic and abdominal surfaces of the diaphram, yet the drainage vessels collect from above and below. The diaphragm occupying a dome-shaped area of considerable extent empties its lymph on the thoracic surface into the lymph nodes that lie in the various adjacent regions. The pleural sac contains lymph vessels that communicate freely with those of the thoracic surface of the diaphragm. The lymph vessels are more numerous at the points of contact of the pleura and diaphragm. Thus the lymph vessels in the region of the aorta, where it passes in relation to the diaphragm, enter these nodes, while the esophageal nodes collect from a more central portion, and the sternal nodes from the anterior vessels. Two of the three areas mentioned contain nodes that join or help to form the mediastinal drainage system. The drainage of the thoracic surface of the diaphragm will depend upon the normal functioning of the nodes on the aorta and esophagus first, and upon the mediastinal nodes second, before the final efferents enter the subclavian veins. The anterior area is drained by the nodes behind the sternum and costal cartilages. These nodes give afferents to the internal mammary chain of nodes that follow the course of the internal mammary artery. We see then that a portion of the thoracic lymph drainage of the diaphragm is collected by the lymph vessels and nodes lying behind the sternal ends of the ribs and a portion is collected by the mediastinal nodes that lie in relation to the aorta and posterior mediastinal glands. The attachment of the outer border of this drum-head-like muscle membrane suggests the possibility of costal lesions affecting its vascular and lymph drainage. The nerves to the diaphragm are given off high up, in the cervical region, and lesions in that area may disturb its innervation. The most probable and most likely disturbance of the lymph flow in the diaphram is through the lymph vessels in the pleura and liver. The presence of septic conditions in the pleura will affect the lymph stream in the diaphragm. The portion of the pleura adjacent to the diaphragm is drained by common efferents. While this is only a small portion of the pleura, yet we find in septic conditions a great amount of lymph blockage and nodular enlargement. The correction of costal lesions and the regulation of the circulation will clear the lymph stream unless there is a great amount of septic poisoning. The abdominal surface of the diaphragm on the right side is in contact with the liver and the communicating lymph vessels are numerous. The subperitoneal tissue vessels also anastomose at the periphery of the diaphragm with its lymph vessels. Here we may again have septic infection through the lymph vessels that anastomose so freely. The aortic nodes collect the lymph on the right side. There are also a few nodes on the inferior phrenic artery. The esophageal nodes, also aortic, collect lymph from the diaphragm on the left side. The esophageal nodes are near the stomach end of the tube. The aortic nodes are to the side and in front of the artery. These nodes have efferents leading directly or indirectly into the receptaculum chyli or lower portion of the thoracic duct. The liver if diseased will reflect its disorder upon the lymph vessels and nodes that drain the diaphragm. Thus we see the diaphragm lies in a position that allows of septic infection through the pleura, diaphragm and subperitoneal tissue. Unless there is a malignant condition in the adjacent
organs and tissues the lymph flow can be regulated through correction of
lesions and the re-establishing of lymph and blood flow. If there
is malignancy it is better to not attempt drainage.
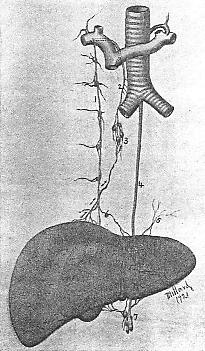
Lymphatics of the Liver As pointed out in the lymph drainage of the lungs and pleura, also of the diaphragm, the collecting lymph vessels drain areas according to the portion of the organ or tissue that is approximate. The liver, having a great surface and occupying a position that for convenience sake we will call horizontal, necessarily must have a lymph drainage that will be divided into parts corresponding with the mediastinal divisions. To make it simple to the student, we will state again that lymph drainage usually follows lines of least resistance, so to speak, and that place is along the course of vessels or of tubes. The hepatic veins lead to the inferior vena cava and we find the lymph vessels from the posterior surface, both deep and superficial, follow along this path. These collecting vessels pass to the nodes around the uppermost part of the inferior vena cava and communicate with the posterior mediastinal nodes. You will remember the short terminal distance the vena cava has after receiving the hepatic veins, also the relation of the vena cava to the posterior mediastinum. The convex surface of the liver that is in relation to the diaphragm has at a few places lymph vessels common to both and we find the nodes on the anterior superior surface of the diaphragm behind the ensiform cartilage collecting lymph for the internal mammary nodes. The under surface of the liver and the bile ducts have lymph vessels that pass to the hepatic nodes and pericardial nodes of a chain that supplies the gastric lymph area. The lymph vessels in the esophageal opening of the diaphragm convey lymph from portions of the liver in that region to the gastric chain of nodes. These are also in communication with the lymph vessels of the pancreas. Thus, we have the lymph vessels passing along the hepatic veins to nodes on the vena cava inferior, others passing through the diaphragm near the front to enter the anterior mediastinal nodes that form a part of the internal mammary chain. The lymph from the under surface of liver is collected by tributaries of the receptaculum chyli directly or indirectly. These latter vessels follow the hepatic artery, bile ducts, portal vein, and through the hepatic nodes. This arrangement makes the lymph drainage simple to understand; the hepatic veins, inferior vena cava, esophagus, hepatic artery, bile ducts and portal vein are all followed by lymph drainage vessels. The lymph vessels pass through the diaphragm at three points. The inferior vena cava opening, the esophageal opening and direct traversing of the diaphragm at the anterior portion to reach the nodes behind the ensiform cartilage. This three-fold system of lymph drainage has various
points of termination. The lymph vessels that follow the hepatic
veins and inferior vena cava are received by nodes that are in the chain
of the posterior mediastinal node group. These nodes have terminals
in the right lymphatic duct unless, as sometimes is the case, they have
separate terminals in the subclavian vein. The second drainage point
is through the internal mammary nodes that have final efferents into the
subclavian vein or the larger right lymphatic duct; the third drainage
vessels are those that are collected in the receptaculum and its tributaries
to be conveyed by the thoracic duct.
PLATE XIX. Lymphatics
of the surface of the liver.
In diseases of the liver we have then three different sets of lymph vessels conveying toxic or possibly septic products. The internal mammary chain of nodes may be blocked or enlarged. This will interfere with the collecting of lymph from the anterior intercostals and the inner surface of the breast, as well as from the deeper areas of the anterior thoracic wall which includes the portion of the pleura in that region. The posterior mediastinal nodes receive lymph that has followed along the lymph vessels in relation to the hepatic veins, and inferior vena cava. Should there be an enlarged condition of these nodes through lung affection, or from any congestion or infection of the various tissues and organs drained by these nodes, we will find the liver flow checked. This may cause other lymph vessels in the liver to take up in part the work of lymph drainage. The third drainage point is through the thoracic duct and here we may find the greatest amount of blockage. The hepatic nodes, the gastric nodes, and the pancreatico-duodenal nodes receive and convey to the thoracic duct a large part of the livers lymph. In gastric disorders, not necessarily malignant, we may look for enlarged nodes, also in disturbances of the pancreas. There may be lymph blockage from a gastro-duodenal ulcer. All these may reflect upon hepatic drainage. The lymph vessels of the liver are numerous and are divided into the superficial and deep, but they all pass through the three sets of terminals outlined above. Eventually they reach the subclavian veins. In malignancy the liver may convey septic products through any of these three separate channels. The puffiness above the clavicles, including involvement of the supraclavicular nodes, mentioned by Osler, as occurring through the internal mammary chain, is not as likely to occur as in the more direct involvement through the other two drainage systems. The posterior mediastinal collect hepatic lymph more direct than does the internal mammary chain and the vessels are from a deeper portion of the liver. These mediastinal nodes send efferents that have a terminal similar to that of the internal mammary chain of nodes and the involvement of the supraclavicular nodes of the former is much more likely. The thoracic duct drainage of the liver lymph is less direct as the lymph must pass through various nodes before being received by the thoracic duct. There is a lessened chance of liver malignancy if we keep the lymph drainage free. We have pointed out elsewhere that the liver is the chief organ in systemic pollution--that in the majority of cases the liver is involved primarily and the other organs are affected secondarily. If the lymph drrainage of the liver is blocked it is only a short time before some other organ will take on a diseased condition. The three drainage systems from the liver include the three systems that also drain the major portion of the bodys lymph. The right mammary chain of nodes collects the lymph of the liver from a small area only. The left mammary chain may receive part of this as the two chains are connected by lymph vessels, but Osler refers to the involvement of supraclavicular nodes on the left side in particular. We find the right side is the important one as the right chain conveys most of the lymph from the anterior diaphragmatic nodes through the nodes back of the ensiform cartilage. The right broncho-mediastinal trunk likewise collects some lymph from the convex surface of the liver. Very little lymph from the convex surface of the liver reaches the left subclavian. The liver has so many vessels and ducts that the lymph stream is well conveyed, but at the same time, there is no organ that blocks itself quicker than the liver. The many functions of the liver and the receiving of the portal vein with its vast distribution and the hepatic veins collecting and emptying into the vena cava, along with the biliary ducts carrying bile into the duodenum, gives us an insight into the lymph vessel blockage that may occur if this organ becomes diseased. The hepatic artery supplying the liver has vasomotor regulation and indirectly the lymph stream is augmented by the normal tone of the artery and its branches. The better the blood circulation the better the lymph flow. Thoracic lesions that interfere with the blood flow to the liver will cause a lymph retardation through the organ. Lesions that interfere with the lymph vessels and nodes between the liver and the subclavian veins must be corrected if we expect good lymph drainage. The left subclavian collects the major part of the livers lymph; the right lymphatic trunk only part from its convex and posterior surface. We must look to the left postclavicular area for
thoracic duct drainage. Cervical lesions, first rib, or clavicular
subluxations may have a bearing on the livers lymph drainage. We
usually think that we reduce an enlarged liver or restore its various functions
to normal by the correction of thoracic lesions at the nerve centres to
the liver, but we must not overlook the lymph drainage which has its terminals
through three different courses before it reaches the subclavian veins.
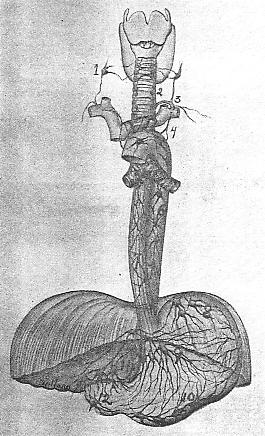
Lymphatics of the Stomach and Intestines In the cardiac lymphatic system we spoke of the lymph flow being accelerated by a constant moving of the lymph vessels located in an organ that is beating almost continuously. In the stomach we have lymph vessels in and on the walls of an organ that has a churning movement and is capable of great expansion through its contents as well as by the presence of gases. The stomach has a goodly number of nodes lying between the folds of the omenta, as well as being distributed around the cardiac end of the stomach, the pericardial, also the pyloric end, the subpyloric. The mucous membrane lymph vessels pass to the sub-mucous. Collecting trunks pierce the muscular coat in the lesser and greater curvatures and these afferents are received by the gastric chain. Efferents from the gastric enter the preaortic nodes of the coeliac group to enter the receptaculum chyli as separate trunks or as the combined channel known as the intestinal lymphatic trunk. After all, the lymph drainage of the stomach as well as of the spleen and pancreas eventually is collected by the coeliac group of nodes which lie in front of the aorta in relation to the coeliac axis. The main lymph nodes and vessels, as in the other organs, lie along the course of the blood vessels. The lymph drainage of the stomach is such that certain areas are drained quite independently of others. This is of value when there is a pyloric diseased condition, the fundus of the stomach may not be blocked or involved. The splenic nodes receive a part of the stomachs lymph along the splenic artery Again we will note, as in cancer of the breast and other organic infectious areas, there may be a regurgitation of lymph. In treating the stomach for a better lymph flow,
we will find it necessary to work with the view of, first, a free thoracic
duct drainage by keeping the terminal clear in the clavicular region, and
second, by a free lymph flow in the coeliac region.
Gastroptosis will prevent gastric lymph vessel efferents from clearing the lymph spaces. As the lymph vessels of the stomach have a common duct drainage with the spleen, pancreas, and mesenteric area, in some instances we must try and determine the amount of blockage that already exists when there is stasis or ptosis of the abdominal viscera. The receptaculum chyli is quite protected by the abdominal aorta and if no aneurism exists or thickened tissues in this region the most important lymph area to note will be that of the preaortic nodes. The reduction of lesioned areas that control the blood vessels that supply and drain the gastric area is of primary importance. On first thought, the student may picture the receptaculum chyli as lying in front of the aorta and subject to gastric pressure and even contact, but we will remember the relation of the aorta to the receptaculum chyli and note that it is the ducts leading to it that are subject to compression and blockage. The diaphragm may be drawn unduly by cervical lesion affecting phrenics, and by lumbar or costal lesions, and this may affect the lymph flow to some extent. The thoracic duct follows along the aorta in its relation to the diaphragm, but lies in a position that is more subject to vertebral lesions. The great proposition in abdominal lymph drainage is one of stasis and ptosis. The entire alimentary tract may have a ptosic expression, a general visceroptosis. About 90% of white people are constipated. The vast majority are slaves to laxatives. Some take oil, others anything from senna to salts. It is easy to reason out the effect constipation has on the lymphatics. The great receptaculum chyli with its numerous tributaries is in a constant state of over taxation. Ptosis and venous stasis are inevitable. The lymph vessels and nodes in the mesentery are chronically enlarged and overburdened. The dragging down of the transverse colon, including the hepatic and splenic flexures, interfere with the drainage of the lymph in the reservoir. Auto-intoxication includes lymph retardation. Toxic accumulation is obvious when ptosis or stasis is present. Splanchnoptosis is one of the vital causes of lymph
blockage. The vasomotor control of the abdominal viscera normally
is possibly one of the best arranged systems in the body.
No organ or tissue remains normal where there is an altered position in the respective regions. Perfect tone is found where vascularization and innervation remains unimpaired. If the intestines are sagged out of normal line the mesentery is likewise malpositioned and the lymph vessels are not free to carry away their load of lymph. There is only one method of correcting stasis and ptosis, and, thanks to the osteopathic technique, we may by adjustment relieve the stress and restore the sagging viscera. We find the spinal column a container of these nerve impulse centers that control not only the circulation but the nerve tone and vermicular action of the alimentary tract. We must look to the correction of lesions and scoliotic conditions for a remedy in abdominal disturbances. First we must correct innominate lesions, if they exist, as it is useless to attempt spinal correction with the expectancy of permanent results without first having the foundation of the spine in perfect alignment. The sacrum must be true to its axis in relation with the innominates. A tilt of the sacrum may be detected when least expected. The limbs must be of equal length, unless a previous break or faulty malnutirion has shortened one. Perfect alignment of osseous tissue first is necessary. Various vertebral and lower costal lesions, so often
found in ptosis, must be corrected as nearly as it is possible before we
may expect a free flow of lymph. The region of the diaphragm is also
very important. An enlarged liver, spleen or pancreas with gastroptosis
must command consideration before we attempt to secure a normalization
of the transverse colon.
Just recently I assisted in an autopsy which gave
me additional data. The case was of peculiar interest as I knew the
subject had been given serum treatment for a duodenal growth. We
spent some time in this post mortem and I examined with care the state
of the lymphatics. Each organ below the diaphragm was overhauled
to determine the amount of lymphatic involvement. It was almost beyond
comprehension. I never knew so many nodes existed. Every node
seemed enlarged and indurated. The jaundiced condition due to duct
blockage, and the gastric outlet almost beyond recognition was surrounded
by a lymphatic enlargement and nodular retention that had defied correction.
If one is sufficiently interested in lymphatics to carefully palpate in every accessable region, it is astonishing how the condition of the nodes will index the patients complications. We have called attention to the fact that no organs containing lymphatics can be involved without a corresponding lymphatic disorder. We may not be able to palpate the lymphatics in all abdominal organs, but in many instances we can learn to detect enlarged nodes or lymphatic blockage. In a measure we can estimate the amount of lymph blockage by the degree of ptosis. We can also determine to a certain extent the lymphatic involvement by the torsion in the duodenum when gastroptosis exists. The question of lymph regurgitation in gastric trouble is verified in operations for duodenal and pyloric constrictions. The relation of the kidneys and suprarenals to the cisterna chyli is also significant. The pancreas, with its peculiar position and relation to the stomach and duodenum, gives us an insight into the lymphatic disturbances found in gastric malpositions. We have a lot to learn yet as to the real part played by the lymphatics in their relation to the ductless glands, but we have come to believe the physiological chemistry of the body is dependent upon the state of the lymph. Faulty metabolism must include a blocked lymphatic system at some point at least. The restoration to health depends upon the degree of lymphatic vessel tone and freedom from obstruction. The nerve centers that control the abdominal lymphatics correspond in a measure to those of the vasomotors to the abdominal blood vessels. Perfect alignment of osseous tissue and reduction of organic congestion will clear the lymph vessels if ptosic conditions are remedied, unless there is malignant trouble. Recently I examined a woman of 53 who complained of gastric disorders. Upon thorough examination I discovered a growth in the region of the duodenum. X-ray confirmed the diagnosis. The case was typical one of lymphatic engorgement. The growth suggested malignancy. Upon reconsideration I decided to pass the case up. The involvement was too great and if malignancy existed it seemed too great a risk to overstimulate the lymphatics. This case was an extraordinary one and in her atonic condition I felt justified in not attempting what might prove a fruitless task. It seems wise sometimes to give in to doubt rather than to face a defeat later and be accused of spreading the toxins. There is a limit to the clearance of lymphatic blockage and it is well to know when to halt. An overtaxed system with constitutional disorders of numerous phases may not be cleared even by the most dexterous adjustment and correction. The lymphatics are sometimes so badly complicated that to attempt to clear them may mean adding fuel to the fire. I have admitted this point just to show how I feel in these severe cases. But the ordinary cases, where no indication of malignancy is present , justify us in attempting at least to clear the circulation and lymphatic glands of their load. In this age when cancer is so prevalent it is well to be on constant guard to detect growths or conditions that indicate an incurable phase. We are laboring to clarify in our minds as nearly as possible the state of the abdominal viscera in their various relations to the benign and malignant classifications. This may not be possible, but we can come nearer to it by study and research. The lymph drainage of the appendix is of particular
value. There is usually at least a node which collects the lymph
from the afferent vessels. We have found that in appendicitis there
is an enlargement of the inguinal nodes of that side. This may be
accounted for in two ways. First, there is sufficient lymph blockage
in this region to cause enlargement of the cecal nodes. The mesenteric
nodes are also enlarged and through the tissue congestion and venous stasis
the lymph stream is checked by an overtaxed drainage centre, the beginning
of the thoracic duct. This reflects upon the emptying of the lymph
from the inguinal region and there is a blocking and enlargement of the
inguinal glands. This may be noted in almost every instance where
appendicitis is present. Second, there are lymph channels in the
inguinal region that have collecting tubes from around the appendix, but
not anastomosing. These lymph afferents are blocked or overloaded
through congestion and disturbed vascularization of the cecal area.
If pus is present in the appendix, the inguinal nodes are more readily
palpable. We have stated elsewhere that surgical resort may be determined
absolutely by the condition of the right inguinal glands. For years
I have based my final diagnosis in operable cases on this finding.
After all other tests are made, the index as to pus finding is determined
by the palpation of these nodes.
Lymphatics of the Kidneys The kidneys lie in a position that is relative to the beginning of the thoracic duct. The lymphatic vessels follow the arteries, as usual, and are of more significance than usually ascribed to them. The numerous lymphatic capillaries in the medulla and cortex have an influence on the tubules. The vascularization of the kidney substance aids the lymph stream in that there are more definite channels than found in some organs. We find that a blockage of the lymph stream in the region of the nodes that receive afferents from the liver, stomach and pancreas reflects itself upon the lymph stream from the kidneys. The blocking of preaortic nodes that receive lymph vessels from the kidneys causes a blockage of the lymph in the cortex and medulla. The effect upon the kidneys is marked, and we have noted that in certain kidney disturbances that normal functioning did not return until the lymph stream was cleared and allowed free drainage from the deeper lymph vessels. Again we note the disturbance of the lymph flow when there is faulty innervation, not only to the kidney blood vessels but to the nerve fibres to the tubules. The lymph stream is influenced by the nerve supply to the vessels and tubules to the extent of causing a variation in the flow of urine. The correction of lesions that have caused instability of nerve tone brings about a more normal flow of lymph, and the organ functions better. A lower costal lesion may cause vascular and lymph irregularities of flow, and derange the finer mechanism in the medulla and cortex of the kidney. Lower thoracic vertebral lesions interfere with the renal plexus of nerves and in this way bring about variations in the secretory cells. We have noted in Brights disease that the lymph stream was blocked decidedly, and that by indirectly influencing the lymph channels through vasomotors to the blood vessels the change in the tubules made repair quite satisfactory. Brights disease is to a great extent a lymphatic disorder. The treatment should be to the end of freeing up the efferent lymph channels in order that the kidney drainage of lymph may be more complete. The collection of the lymph from the superficial vessels is of less importance. The channels eventually end in the nodes around the aorta and the lymph is collected at the beginning of the thoracic duct. There are so many lymph nodes and vessels in this small area that it is reasonable to expect an overtaxed condition of the nodes if there exists any organic disease of any of the adjacent organs. The blockage of the nodes and channels from the stomach or mesenteric region will have its influence upon the renal lymphatics. Ptosis of the stomach will also have a bearing. Correction of all lesions to this area will relieve the kidneys and make the urine more normal in color and quantity. We have never paid sufficient attention to the lymphatics of the kidneys in the various diseases of these organs. While diabetes is a constitutional disturbance, we find the liver and kidneys almost invariably taxed and the renal lymphatics blocked. If you apply specific treatment to the lymphatics in diabetes you will get good results. The hepatic nodes and renal nodes, as well as the mesentery, must be kept free from blockage. If they are blocked you will soon see it reflected upon the drainage of the pelvis and even the inguinal and popliteal nodes. The lymph drainage below the kidneys will not be normal if there is enlargement of the nodes and blockage in the lymph channels in the region of the receptaculum chyli. First we must work to secure good vasomotor control of the branches of the abdominal artery, also the corresponding collecting veins. If we secure this, we can reasonably expect an effect upon the lymph drainage. The lymph vessels follow the blood vessels so closely that we can usually aid lymph flow by vasomotor control of the blood vessels. We are yet to determine just how extensively vasomotor fibres are scattered over the lymph vessels that are so closely associated with the blood vessels. We are inclined to believe that there is more influence brought to bear than we have given credit for. A little further research work will clear this point. We are also yet to determine just how much lymph is collected in the veins over the body outside of the subclavians. As mentioned elsewhere, we believe that in time we shall determine that the entire venous system collects lymph at numerous intervals, as it seems incredible that the entire lymph collection of the body should be confined to the two veins in the base of the neck. If this reasoning is true, it will account for the clearing up of the lymph stream when we secure normal vasomotor control of the blood vessels. The close relation of the lymph vessels and nodes to the veins in many instances allows for collection of lymph in the veins at various point in minute quantities. This is a solution to the problem of the lymphatics in various conditions where there is a lymph blockage and an edematous condition. PLATE XXIII. The lymnphatics of the kidneys. The lymph drainage of the kidneys is most important in any and every systemic disturbance. The degree of normal functioning of the kidneys means the blocking or clearing of the other tissues and organs. Specific treatment to increase lymph flow in the vessels leaading from the kidneys is most essential. The internal secretions are influenced by the lymph more than in any other way. Every organ has a blood supply, and along the vessels we find lymphatics with few exceptions. In order to stabilize the body metabolism we must secure perfect lymph drainage. This will allow ductless glands as well as all glands and tissues to put forth normal secretions. The nodes must be kept reduced to normal size and the lymph channels free. There are enough palpaable glands to serve as an index to internal systemic disorders. No organ or ductless gland can be involved to any great extent without reflecting its disturbance and blockage on some palpable area. We must look for edematous areas. There are cetain areas that denote specific organic lymph blockage. The watching of these regions that are prone to puff is very essential. Learn to detect puffy areas. They may exist on most any part of the body. There may be zones that are puffy and cool to the hand. Trace out the lymph drainage and you will locate the organs with blocked lymphatics. If the kidney lymph drainage nodes are blocked you
may find a general edema over the kidneys in the back, or it may be reflected
on the abdomen over the beginning of the thoracic duct. Next go above
the clavicles and note any edema, and by comparing the three areas you
can pretty well decide the drainage of the kidney lymph. If there
is a splanchnoptosis present it will be necessary first of all to correct
lesions that will allow a return to normal position of the viscera.
General alignment will be necessary from the arches of the feet upward
to the atlas. General vasomotor tone of the body will greatly accelerate
lymph flow. Specific work in one area will not always clear the trouble.
The lymphatic system must be considered in its entirety, and we must work
to the end of freeing the lymph channels, nodes and ducts in order to reach
some specific organ or tissue.
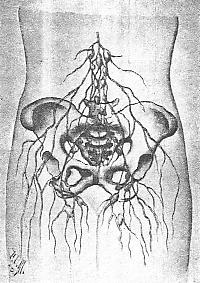
Lymphatics of the Pelvic Region The organs in the pelvic basin are subject to great stress when innominate lesions exist, and such lesions are not uncommon. Even one innominate in lesion will draw out of line the uterus and ovaries. This unevenness of the basins walls causes muscles and ligaments attached to the innominate bones to draw in a manner that blocks the blood vessels and lymph channels. Nodular enlargement follows, and a congestion of the tissues is also noticed. If allowed to remain uncorrected, marked symptoms appear, especially at the menstrual periods. Cramps, retarded flow, and sometimes flooding are the result, depending upon the age and general condition of the patient. As long as osseous lesions exist there will be blockage of blood and lymph vessels. Careful palpation over the ovaries will reveal the change in the tissues. The effect upon the lymphatics in the legs will be apparent. There may be a slight edematous condition around the ankle, and the popliteal spaces are sure to record the blockage that is present higher up. If the kidneys are active and no constipation is apparent the symptoms are minimized, but in a tilted pelvis there is almost sure to be constipation of haemorrhoids. There is stress upon all the muscles attached to the pelvic basin. The lymphatic arrangement in the pelvic organs is like that of a great net. These vesesels all find an emptying place eventually through one tube, the thoracic duct. This duct collects from all points below. The uterine and ovarian lymphatics are blocked when there is undue pelvic congestion. We need not refer to venereal diseases and then marked effect upon the lymphatics. We will confine this article to pelvic lymphatic blockage, through lesions, with resulting ptosis and nodular enlargements. In order to have a regulated blood supply in the
pelvic organs there must be good vasomotor tone at the nerve centers that
control the blood vessels, and indirectly the lymph vessels. Cervical
and thoracic lesions affect vasomotor control clear down to the feet.
Weakened ligaments allow misplacements, and we find flexions and versions causing nodular enlargements. Varicose veins and edema follow in many instances. If there is a continued lymph blockage in the ovarian and uterine regions, leucorrhea may be the result and often is very persistent. The vascular and lymphatic arrangement is peculiar in the pelvic basin. This allowance is made to accommodate the changes during pregnancy. The lymph vessels are arranged so that the gravid uterus will not obstruct them sufficiently to cause white swelling under normal conditions. Pelvic and vertebral lesions existing before and during pregnancy cause many symptoms that would not exist had the lesions been corrected before conception. Where there is albumin during pregnancy, we find the lymph nodes more noticeable and the lymph drainage down the leg more blocked than in a normal kidney condition. Before any woman contemplates pregnancy there should be perfect adjustments made, and a free drainage of the pelvic lymphatics. The presence of lacerations, long neglected, are causative of nodular enlargement. The absorption of secretions and discharges reflect the abrasion upon the nodules. This may produce sufficient nodular enlargement and lymph blockage to cause intrauterine growths. Any abrasion is followed by lymphtic disturbance. In cases of a prolapsed uterus we find stress upon
the numerous lymph vessels and nodes, preventing the return of lymph through
the tributaries of the receptaculum chyli. Constipation with enlargement
of the haemorrhoidal veins produces a nodular enlargement that is readily
palpable in the posterior walls of vagina, especially back of the cervix.
During the menstrual period there is a temporary
lymph stasis and you will notice, sometimes, the inguinal nodes slightly
enlarged and yet quite compressible to touch. These clear up shortly
after the period.
If you will keep the lymphatics in mind constantly and look for nodular variations in all disorders of the organs and tissues, you will be surprised in time to note a peculiar fluctuation of the various palpable nodes in the accessible regions. I have become so accustomed to palpating nodes that I invariably go over the popliteal, inguinal and axillary regions, just to satisfy myself that the lymphatic system fluctuates, so to speak, according to the chemistry of the body. The slightest organic disturbance reflects itself upon the lymphatic system at some point. An abcessed tooth, an enlarged tonsil, a bronchial cough, a ptosis or stasis in the mesentery, a pelvic congestion or organic prolapsis, all record themselves on the lymphatic system that becomes blocked so readily when poisons or toxic products are found within the system. Enlarged lymph nodes are a true index of some pathological phase at some point within the body. There is a communication between the lymph vessels of the uterine area and the superficial inguinal nodes. This allows of more ready palpation of the inguinal nodes in a case of diseased uterus. The majority of the lymph vessels of the uterine walls and coverings follow along the broad ligaments. The aortic nodes eventually collect the lymph. The iliac nodes collect from the cervix, according to the direction of the various lymph vessels from that part. The vagina is lymph-drained by the nodes that lie along the iliac vessels and their branches. The lymph drainage from the bladder is separate from that of the vaginal region until the iliac nodes are reached. On the sacrum we find a few nodes which collect with the mesenteric nodes the lymph from the muscular coat of the rectum. The lymph vessels follow the course of the haemorrhoidal vessels where nodes are distributed that send efferents to the mesenteric. The sacrum, if tilted in relation to the innominates, may disturb these lymph nodes. |
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}