
|
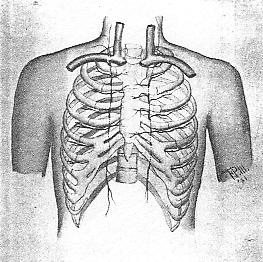
The Lymphatics of The Lungs and Pleura The most perplexing part of the lymphatic system to a student is possibly that of the thoracic region. It is easy to understand the thoracic duct and its cluster of tubes at the lower part, the cysterni chyli, but the drainage of the intercostals, the lungs, bronchi, esophagus, heart and diaphragm is difficult to comprehend. There seems to be a lack of plates in most texts on anatomy to furnish object lessons. In a general way a few of the channels are shown, but the student is still at a loss to comprehend just how there may be ducts that convey lymph from these various organs and tubes as the bronchi, esophagus and aorta, and still be independent of the great thoracic duct. Let us open this discussion by saying that the lymph must eventually reach the subclavian veins, or possibly the innominate veins. The student is familiar with the fact that the lymph flow to the subclavian veins empties through two main ducts, the right lymphatic, and the thoracic duct. There are other points of entry separate from these two main ducts; sometimes two or three. For instance, the internal mammary ducts usually empty into the subclavian as distinct ducts. The mediastinal may join the mammary or empty separately, but they all enter the veins at some point within a small radius. It may be on the upper surface, the anterior, or even inferior surface of the vein. Now let us take up the drainage of the bronchial nodes first. Around the lower part of the trachea and over the surface of the bronchi the tracheo-bronchial nodes are scattered. At the angle of the bronchi and also where the bronchi divide nodes are present. They even extend to the bronchioles but not into the alveoli. All of these nodes have efferents and must be drained. The drainage is upward toward and into the subclavian veins. These nodes drain the lung tissue as well as the bronchi and trachea. The lymph from the heart reaches these nodes also in part at least. The efferents from these nodes join in some instances those of the internal mammary and pass on to the subslavian veins. The right may enter the right lymphatic duct, or may enter the subclavian vein direct. On the left side the thoracic duct may receive the mammary efferents or the subclavian vein receive the drainage directly. The lungs have their superficial and deep plexuses of vessels, but they all drain towad the yilum which receives the lymph flow of the lung tissue. From these nodes the tracheo-bronchial nodes collect and through their efferents eventually empty into the internal mammary or mediastinal nodes to be conveyed to the veins on either side. The superficial and deep lymph vessels in the lungs anastomose only at the hilum, at the root of the lung, on either side. The pleura has a more distinct drainage as the visceral layer drains into the lung afferents on its surface, while the parietal lymph streams are collected according to the regions they are located in. In front they are collected by the internal mammary after passing through the intercostal muscle lymphatics, while the lower parietal lymph vessels may join with the vessels of the diaphragm. In the posterior region the mediastinal nodes collect the lymph from the parietal part of the pleura. PLATE XVI. The internal mammary lymph chain collects lymph from the anterior intercostal spaces, inner areas of breasts, some from the pleura, and from the upper anterior surface of the liver. Thus we see how simple the drainage is if we remember
the collecting tubes of the different regions.
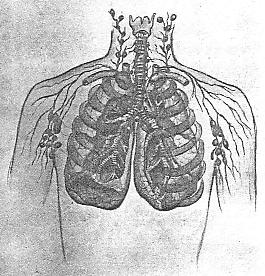
In the first place, we wish to emphasize the importance of free lymph drainage in the nodes that collect and send forward the lymph. We have mentioned in another chapter the fact that lung infection is usually downward from the throat. It is easy for a catarrhal condition to work its way downward, also infection and congestion. The nodes in children are of a pinkish tint, but in the adult they often become dark or black and enlarged. If these blocked nodes become infected with tubercular germs, suppuration may take place, and the discharge may be thrown into the bronchi. This will infect the lung tissue in time, as only part of the discharge can be coughed up. The breaking down of the nodes is often the result of dust laden particles being conveyed to the bronchial tubes. Now, we come to the osteopathic idea of keeping these nodes in tone. We cannot keep people away from dust and irritating inhalations, but we can keep the pulmonary and bronchial vessels and tissues toned up through our method of adjustment. The contour of the chest wall may have a lot to do with the condition of the blood and lymph supply within. A flat-chested person has not the chance for resistance that a well rounded chest has. The sagging of the ribs may be due to lack of tone in the muscles, but we find that more often there is either a curvature or one or more lesioned areas. To correct posture we must first secure spinal alignment. We may have to start at the innominates and work from that basic standpoint. As we secure normality of the spine, we can elevate the ribs and secure better vasomotor control. Adjustment of the upper thoracic area will add tone to the lung tissue as the circulation will be more regular. Where we secure a good arterial supply we also insure a better venous drainage. We are now reaching the point where we can work to advantage on the lymph stream. We pointed out the various drainage tubes, and it is to the end of securing a better lymph flow that we now work. The nodes are secondary in importance in some respects to the efferent flow of lymph. Unless we have a free drainage we cannot expect to relieve the over-burdened lymph nodes. If it were possible to keep the thorax in normal position, vertebrae, ribs and sternum, we would have little difficulty in regulating the blood supply. The good blood coursing through the vessels and tissues would sustain a tone that would prevent germs from gaining a hold on the nodes. The nodes are usually normal if the blood circulation is perfect or nearly so. You will recall the generous blood supply that most nodes have. It is this supply that keeps the nodes capable of resisting invasion. If we work to the end of regulating blood supply to nourish and drain, vascularly, the nodes, we will find we have accomplished much. The sinuses within the nodes are kept normal mainly through the blood that supplies each node. Here is where we check the points of invasion. A node breaks down because it has lessened resistance through faulty circulation of the blood. Thus we have the proposition of keeping up the tone of the lymph nodes and vessels through vasomotor control of the blood vessels. This point is seldom if ever emphasized, but it holds good in any part of the body where nodes exist. The entrance of dust, irritants, poisons, germs or foreign substances of any nature into the nodes may be offset to a large degree by the regulation of the blood supply to and from the nodes. PLATE XVII. Lymph drainge of the larynx, trachea, bronchial tubes and bronchioles. In weak-chested people we must first of all secure alignment, then good posture, and finally good tone through indirect vasomotor control. The efferents from the pleura include the internal mammary, as we have said. The internal mammary receives part of the intercostal drainage. If there are one or more costal lesions a proportionate blockage will result. If the scaleni muscles are tensed through cervical lesions, and the first and second ribs drawn upward, there is a possibility of interference with lymph drainage from a portion of the lungs and pleura. The vessels crossing the first ribs may be interfered with and the thoracic duct on left side drawn in a position to check drainage into the vein. The vessels to the bronchial tubes and lungs are controlled through vasomotor centres that may be influenced in the upper thoracic sections. The nerves to the lungs may be influenced by cervical lesions as well as upper thoracic. Blockage of the lymph stream in the neck or around the trachea may interfere with the lung efferents. The tracheo-bronchial nodes and the mediastinal may be checked in their drainage through congested membranes and tissues. This calls for a better vascular regulation. These two systems work together to clear any area or region. We must work to secure good lymph drainage by not only removing any interference with the effervents from the nodes, but through the reducing of congestion around the nodes and efferents. The clavicles have much to do with interference with lymph drainage at times. We find a clavicle in some instances not in true alignment, occasionally backward at external end. It is well to see that they are not drawn out of line. There are so many vessels, nerves, tubes, etc., passing through the upper thoracic opening that we need to determine if there is room for these various structures; also, note the presence of congested or thickened areas. The person with a goitre may have a weak-chested condition not only through disturbed nerve impulses, and irregular blood flow, but by lymph blockage as pointed out in the chapter on the thyroid gland. The broncho-pulmonary nodes are usually over-burdened at their best. It is a question whether any one has normal nodes in this region. Inhalations and catarrhal exudates and infections by tubercular germs, even though practically latent, all contribute to keep the nodules in the region of the hilum in an overtaxed state. The alveoli have no nodes, but the lymph vessels are found in the lung tissue. The correcting of lesions that will insure better respiration will do much to clear the lymph vessels. Any interference with the intercostal muscles or costovertebral attachments will shorten breathing and correspondingly impair lymph drainage. Very few people breathe properly, and when they contract colds or have a cough they almost immediately assume a faulty posture. This drooping of the chest not only affects the intercostal lymph vessels but retards the flow of lymph in the thoracic duct and mediastinal nodes. The erect posture relieves the pressure and the efferents convey their lymph more readily. We have not given the lymph flow sufficient thought in the past. We have never realized the full significance of free lymph drainage. The lymphatic system peripherally being a blind end or closed system, we have felt that it simply cleared itself according to the physiological activities found in various conditions. The lymphatics start their collecting system in the capillaries and it is only through indirect tone furnished by the tissues and vasomotors that control the vessels that we can expect a normal flow of lymph. Only the numerous valves prevent the lymphatics from becoming thoroughly blocked. At all times work to secure good lymph drainage. By so doing you invariably at the same time secure better vascular regulation. The lymph stream is the weak member in the circulatory system and we must study out every method of securing better drainage of lymph in order that the nodes will not become blocked and indurated. We depend upon the lungs to purify the blood but we must not forget that there is a separate set of blood vessels that supply the lung tissues, and that these tissues must be drained also by not only the veins but the lymphatics. Unless we can keep the broncho-pulmonary lymph nodes clear the aeration of the blood in the alveoli and lung tissues, will not be sufficient to prevent breaking down of the general system through a checking and final infection in the nodes around the bronchi. The aeration of the blood in the lungs is no more important than the preventing of induration in the nodes that drain the lung tissue. To have good general circulation and tone throughout
the body we must have cleared afferents and efferents in the broncho-pulmonary
nodes.
Lymphatics of the Axillary Region The physician is more familiar with this region, lymphatically considered, than any other except the cervical. It is so common to find enlargement of the axillary nodes in infectious diseases and after vaccination that his attention is called to this area frequently. The possibility of lymph blockage at this point makes one think of the efferents that lead to the subclavian nodes. These nodes empty by vessels on the right side into the subclavian vein or directly into the right lymphatic duct. Between the subclavian nodes and the terminal drainage point the subclavian trunk passes between the vein and the subclavius muscle, and then behind the clavicle. On the left side the trunk may enter the thoracic duct or empty directly into the subclavian vein at the junction with the jugular. The subclavian muscle may be in a state of tension from a subluxated clavicle or through disturbed innervation of the muscle. These lesions will retard the flow of lymph in the vessels. When we consider the deep lymph drainage of the axillary region, its drainage of bone, periosteum, ligaments, muscles and other tissues, we get an idea of the relative importance of keeping all muscular contractures at a minimum. If there are costal lesions they will affect lymph drainage, and if the pectoral muscles are tense, we must expect a similar retardation of lymph flow. The free anastomosis found in the lymph vessels of the arm, as elsewhere, makes the lymph drainage of the axillary region a common one. The central group of nodes in this region collect from a vast area and the point of interest lies in the direction of the terminal drainage point. The supraclavicular and the subclavian nodes are often blocked. Even the lower cervical nodes are involved when the axillary are enlarged. Snow refers to regurgitation in malignant case leading to retrosternal involvement and secondary infection of the head of the humerus. We find regurgitation possible elsewhere as in the lymph vessels in gastric cancer. This simply proves that although lymph vessels have numerous valves there may be regurgitations under certain conditions. Going back to the lymph drainage of the muscles we may reach and influence the flow of lymph through a better vasomotor control of the blood vessels that supply the tissues and nodes. We may also reach the lymph drainage through correction of lesions that remove muscle tension over and around the lymph vessels and nodes. This will call for adjustment of the cervical region to insure normal tone in the brachial plexus. Correction of upper thoracic and rib lesions will stimulate vasomotor and trophic centres. Costal correction will regulate the upper thorax so that the lymph drainage into the subclavian veins will not be checked. The scaleni may be overtensed through cervical lesions. Correct posture will help to insure good lymph drainage from the axillary region. The lymph vessels and nodes often are attached to the sheath of the veins. They follow the vessels closely in many instances. This is another reason why we should keep muscle tension at a minimum, as a tensed muscle will interfere with the blood flow and a thickening of the adjacent tissues may block the lymph flow and cause an undue toxic effect that will result in a blocking of certain lymph nodes and vessels. The axillary region is an active one in that the use of the arms cause the muscles of the shoulder and pectoral region to be actively engaged. Normally muscular activity aids lymph flow as well as venous flow. It is when there is axillary adenitis or lymph blockage in the afferents that motion is sometimes disadvantageous to the lymph stream. The mammary area, if blocked, will check the flow in many of the vessels. If there is an additional axillary blockage the regarded mammary lymph flow will cause a pectoral disturbance that will not clear until the axillary and subclavian nodes are reduced. The subclavian may receive mammary lymphatics, also the internal mammary nodes will take up part of the mammary drainage, but it is through the axillary nodes collecting the pectoral lymph that we must look for drainage when we find tumors forming in the breast. We are called upon almost constantly to reduce these lumps. If there is no malignant condition we are reasonably sure of reducing them by axillary drainage unless they are unduly indurated. The lessening of pectoral muscle tension and correction of costal lesions, as well as cervical and upper thoracic lesions, to insure normal nerve tone, will be the more important. Direct manipulation of the axillary nodes is contraindicated. It is far better to reduce node enlargement through adjustment of lesions as outlined above. Sometimes a lymph vessel from the mammary gland passes through the substance of the pectoralis major leading to the subclavian nodes. If there is faulty innervation to this muscle the undue contraction may check the lymph flow. The region of the scapula is drained by efferents into the axillary nodes. We now see what a large area these nodes in the axilla collect from. In cases of scoliosis, where there are group costal lesions, we may find a sufficient blockage to over-burden the nodes of the axilla. If there is a goitre, and the lower cervical nodes are enlarged, we may find an additional pectoral blockage, especially if the lymph vessels of the upper extremity empty into the two large terminal trunks, the right lymphatic and the thoracic. It takes but very little supraclavicular edema to interfere with terminal drainage. The entire arm may be affected. Slight puffiness around the fingers may lead us to suspect lymph blockage either in the axillary or clavicular regions. The small nodes in the cubital fossa, or the epitrochlear nodes may become enlarged if there is interference above. The establishing of better circulation in the arms by vasomotor tone will assist in clearing up a lymph sluggishness. The cervical area must be cleared first. The first dorsal nerve must not be overlooked as a branch of that nerve enters in the nerve plexus. The first rib is sometimes slipped sufficiently to cause a lymph disturbance. Test out the arm movement to be sure that the tendon of the biceps is absolutely in the groove, and that there is a good free arm movement. Neuritis is so common that we find many mild cases in every day practice. Well-marked cases are fairly common also. The lymph flow, if checked, will poison or irritate the nerves as there is a certain amount of lymph fluid within the sheath of the nerve. In fact, I am inclined to believe that neuritis and tic are lymphatic disorders. In experimenting with both of these maladies we have found that there is always a lymphatic involvement, and that, upon freeing the lymph flow, the symptoms disappear. This statement may be new. I have not seen it discussed elsewhere, but if you will work on lymphatic drainage technique in these two troubles, you will soon find that the lymph flow that has been checked for a period of time has much to do with the unpleasant symptoms that are associated with it. Secure good venous drainage and then work to the end of reducing the nodes by treatment around the base of the neck. We will take up intercostal lymph drainage in the
next section. The pectoral lymph vessels anastomose with the intercostals
at some points, but axillary drainage does not include intercostal drainage
to any great extent.
Intercostal Lymphatics The intercostal area is extensive. The combined length of the intercostal arteries and veins would measure possibly 72 feet. The lymphatic vessels have nodes principally at the sternal and vertebral ends. A few nodes may be found in the intercostal spaces. The posterior nodes of the intercostal lymphatic chain lie near the heads of the ribs and receive the afferents from the intercostal spaces and muscles. The upper five or six nodes have efferents leading to the subclavian veins in the two main ducts. The lower six nodes have efferents leading to the beginning of the thoracic duct near the receptaculum chyli. Thus the drainage of the posterior and lateral sections of the intercostals is partly upward and partly downward, and then upward. The right lymphatic duct receives only the efferents of the upper six intercostals in the posterior region on that side, and the thoracic duct the upper six left at its terminal into the subclavian vein and the lower six, right and left into the beginning of the thoracic duct. About eighteen intercostal efferents of the posterior thoracic region enter the thoracic duct at some point and only six the right lymphatic duct. The anterior intercostal drainage lymph vessels are in relation to the internal mammary blood vessels. The internal mammary nodes collect and carry lymph by efferents to the subclavian veins. They collect from the thorax, mammary bland, upper surface of the liver, the diaphragm, internal intercostal muscles, and subpleural tissue. So we have two systems of drainage of lymph in the intercostal region, and two chains of nodes, one on front of ribs near costovertebral union, and one behind sternal end of ribs in relation to internal mammary blood vessels. The two chains on either side of the sternum in the anterior region have efferents from their nodes to the subclavian veins. Each side draining into the vein on each side as compared with the posterior lymph drainage of three fourths into thoracic duct and one fourth in right lymphatic duct. The nodes found behind the sternum at the lowest point collect from the diaphragm and the upper surface of the liver and pleural surface in that area. It is through the anastomoses of these two anterior chains and their collection from the outer mammary region that infection may cross from one side to the other in malignant breast cases. It is also through the lower collection of lymph back of the ribs in the sternal end that diseases of the lungs and liver may be conveyed from one organ to another. The lymph vessels from the parietal pleura enter these nodes. The many lesions that may interfere with intercostal lymph drainage hinge principally on the lack of normality of the spine. Single or group lesions of the ribs will interfere with lymph drainage. The first rib may cause more disturbance than any other, as it is in relation to the subclavian vessels and these veins receive the terminal drainage of all the lymph. So, we will start at the top; first, we will detect any subluxation through scaleni tension or through costovertebral tension. Next the upper thoracic vertebrae to determine existing lesions, three vertebrae usually, at least. A single vertebra is seldom in lesion without disturbing the one above and the one below. The intercostal nodes near heads of ribs may be enlarged through the state of the tissues supplied by the intercostal blood vessels, through lesioned ribs, or vertebrae. These nodes are usually independent of communication with the mediastinal nodes and vessels. They simply drain the lymph from the intercostal spaces and convey it to the subclavian veins. The internal mammary nodes receive the lymph vessels of the pleura in that region and connect with lymph vessels of the diaphragm and the upper surface of the liver. These last nodes and efferents may eventually join the tracheobronchial and anterior mediastinal to form the brochomediastinal that empty into the subclavian vein directly, or into the large ducts on either side. The second rib may also be lesioned, by contraction of the attached scalenus muscle, or by a vertebral lesion. This rib, with the first, forms the uppermost intercostal space. The lymph flow will be interfered with if there is undue intercostal tension, as by separation of the two ribs through stress or lesion, and lymph blockage may occur if the ribs are approximated through vertebral lesions or costal subluxations. The postero-lateral intercostal lymph vessels follow the blood vessels, as is the rule elsewhere, and the lymph drainage may be interfered with, secondarily, by the blood supply being checked, or through venous stasis by lack of vascular drainage. So we might go on, rib by rib, and discuss each intercostal space, but suffice it to say that single rib lesions may cause a greater proportionate disturbance than group lesions where there is an extended scoliosis of gradual development. In any instance, however, we are interested in the lymph flow, and especially the efferents that convey the terminal drainage. The thoracic nerves are nourished by a regulated blood supply. The lymph enters into the drainage of the tissues and the channels must be kept clear if we wish tone in tissues supplied with blood. Faulty posture and a drooped chest will not only affect the intercostal venous and lymph drainage but may block the veins and lymphatics of the organs both in the chest and below the diaphragm. We cannot have a blockage at any point between the terminal lymph ducts and a more remote area without a checking of the lymph flow beyond the point of blockage. The proposition is similar to that of the blood stream. Impaired intercostal drainage will prevent hepatic, pleural and diaphragmatic lymph flow. In fairly normal conditions the interference with lymph flow at any point may not mean systemic disturbance, but if there exists inflammation as is found in certain organs and coverings when certain diseases are present, we find the collateral anastomotic lymph vessels conveying and spreading the toxic products, and in malignant cases regurgitation in some instances, as referred to in another section. In certain dissections we have observed nodes more numerous than found in bodies where no malignant conditions exist. In the epigastric region especially the blockage in the venous tissues and the resultant thickened tissue, through congestion and toxic deposit, there are numerous small nodes and disturbed lymph afferent and efferent vessels, which allow a more widely spread toxic condition. The lack of rib movement in certain cases where the spinal and costal muscles are almost rigid through colds or lesions or even organic reflex irritation, all point to a checking up of the lymph flow in the intercostal vessels and nodes; also in the trunks leading to the subclavian vessels. There must be freedom of chest movement, as mentioned by Dr. Bush in her chapter on exercises, if we may expect free lymph flow in the afferents. There must also be motion in every thoracic articulation to insure intercostal lymph and blood flow. The vasomotors that control the intercostal arteries have an indirect influence on the lymph flow. The better the blood circulation in both arteries and veins, the more normal will be the lymph flow. A subluxated rib may affect the lymph flow sufficiently to cause poisoning of the tissues around a nerve. Thus we see in herpes a breaking out on the skin due to a lesion affecting the nerve and its sheath. In almost every instance an osseous lesion will cause a lymph disorder as well as vascular irregularities and nerve instability. The lymph spaces are almost everywhere and they must be reckoned with if we wish healthy tissues. Wherever there is muscle rigidity or tension we will find the lymph spaces and vessels more or less blocked by undue tension and altered vascularization. The lymph flow must move onward just the same as the venous blood, or there will be pathological changes as a result of the inactivity. The lymph passes through nodes continuously in a normal tissue condition. The checking of this flow through any of the causes that interfere with the nodes activities, or of the lymph vessels conveying properties, will mean a changed lymph substance. If the nodes collect and retain lymph laden with toxic products, suppuration will result. Should this occur in the bronchial nodes, there is danger of tubercular infection in the lung tissue from the broken down nodes that lie along the branches of the bronchial tubes. If the nodes in the mammary gland become enlarged and indurated and then malignant, through adjacent tissue and duct poisoning, there is danger of spreading of this substance through the lymph vessels. The lymph must be conveyed to the subclavian veins without nodular retardation to be good lymph. The moment there is a checking of the lymph flow in the vessels or nodes, that moment the lymph is altered in its consistency. The influence on the immediate tissues surrounding a blocked lymph node may be observed in palpable areas, and if there is continued blockage and nodular enlargement, the other nodes and vessels may cause the disorder to become a systemic one instead of local. The whole system of lymphatics may become altered
eventually, through a primary pathological area in which there has been
retained toxins followed by suppuration.
Lymphatics of the Heart and Pericardium The relation of the heart to the trachea allows lymph drainage of both to readily enter the tracheobronchial nodes. The plexus of lymph vessels in the endocardium communicate freely with the plexus found inside the visceral pericardium. The efferents follow the coronary vessels in the grooves on the surface of the heart and the right and left vessels pass backward in relation to the pulmonary artery to reach the trachea and bronchi. The lymphatic drainage of the heart is worthy of
special consideration. Here we have an organ in a class by itself;
a moving organ, pulsating and pumping blood all over the body after receiving
it, with valves opening and then closing. The lymph vessels are moving
also with the heart in motion, and they are also influenced by the constant
contraction and relaxation of the cardiac muscle. Possibly nowhere
in the body do we find a better lymph flow than in the heart, and its covering,
the pericardium. The absence of nodes is explained by the active
drainage through the efferents. Nodes are practically unnecessary,
and if present might, in certain cardiac disorders, cause undue pressure
and disturbance to an organ that is sensitive to pressure or stress.
The lymph spaces between the bundles of cardiac muscles in the connective
tissue communicate with the vessels in the endocardium and epicardium.
Thus we have normally a perfect drainage of lymph from the heart to the
nodes on the trachea and its divisions. It is through a blockage
of the tracheobronchial nodes that we find interference with the lymph
flow in and around the heart. In tubercular conditions of the lungs,
when there are enlarged tracheobronchial nodes and suppuration, a secondary
effect upon the heart is noticed. The cardiac efferents no longer
drain the lymph freely into the nodes and terminal efferents. There
is a tendency toward coronary vessel thickening and hardening. In
angina we find the lymph drainage has been checked and a deposit formed
that is due to continued lymph blockage. Again we find the cardiac
nerves affected by lymph blockage and node enlargement in the areas where
the nodes are adjacent to the cardiac nerve trunks. The cervical
cardiac sympathetics as well as those coming from the pneumogastric may
be compressed by poor lymph drainage in the cervical nodes and vessels.
There may be an edematous condition of the tissues in the neck and throat
due to lymph blockage that will reflect itself upon the base of the heart
and the superficial and deep cardiac plexuses. The lesions that cause
vasomotor instability of the coronary arteries and blood vessels leaving
the heart, pulmonic and systemic, may influence the lymphatics in the walls
and around the heart. The blood supply to the various cardiac nerves
and plexuses may cause a change in the lymph spaces which, in time, will
produce a slight cardiac variation of rhythm. This has not been accounted
for in the various treatises on heart diseases, but we have found that
the lymphatic system plays a goodly part in the rhythmic action of the
heart. In one case treated some months ago, when an accelerated cardiac
action existed, we noted a lymph blockage and nodular enlargement in the
cervical region accompanied by edema in the supraclavicular area.
Desirous of regulating the hearts action by a better lymphatic drainage,
we worked to that end. Reduction of cervical nodes and a better drainage
of the efferents from the tracheobronchial nodes brought about a more normal
heart action in a very short time. We assumed that the lymph spaces
were more or less blocked in the cardiac muscle tissue and poisoning or
irritation had existed through lack of free drainage of the lymph in the
right and left trunks that go to the tracheobronchial nodes. The
lymph had been retained too long, and the effect upon the cardiac muscle
was observed. The cervical area also had its influence on the cardiac
nerves through lymph inactivity, and the edematous area above the clavicles
aided the blocking of the lymph flow from the lower nodes and efferents.
Too little attention has been paid to the lymphatic
consideration in relation to heart action. Hardening of the coronary arteries
is a lymph proposition to a great extent, and the primary lymph blockage
may be at a distant point. The effect of costal and vertebral lesions on
the flow of lymph has been discussed in another section, but we wish to
emphasize again the importance of free lymph drainage through the correction
of lesions that will block the lymph flow from the tracheal region and
cardiac efferents. Very little lymph flow interference in the auricles
and ventricles will in time cause a cardiac fluctuation from normal. We
may look for this in cases where there is bronchitis and nodular enlargement
above the clavicles.
Lymphatics of the Esophagus This tube is of sufficient length to have at least two collecting systems of lymph vessels. We find the network of lymphatics in the muscular coat collected by the submucous. They collect from the lymph spaces in the mucous tissues and in the lower part of the esophagus the drainage is toward the nodes in the coeliac region. In the upper part of the esophagus the posterior mediastinal nodes receive the afferents and convey the lymph by efferents to the subclavian veins. The esophagus is drained then by nodes that lie adjacent to the tube. The flow of lymph depends chiefly upon the normal activity of these adjacent nodes. The lower drainage will depend upon the patency of the thoracic duct that indirectly receives the lymph vessels from the esophagus. It is the upper drainage that is the more important as all of the lymph must eventually reach the thoracic duct and subclavian vein in some way. Should there be bronchial affection and enlarged nodules in the posterior mediastinal area, the lymph checking will be reflected upon the drainage of the esophagus. The vasomotor control of the blood vessels to the esophagus will indirectly act upon the lymph vessels. Lesions that cause a vascular irregularity in the esophageal tissues will block the lymph spaces and cause retarding of lymph that will produce a change in not only the mucous tissues but in the lymph fluid. Retardation of lymph in the lymph spaces for any period will cause changes that in time will interfere with the normal action of this tube. The nodes that collect the lymph from the esophagus also collect the lymph from the diaphragm, upper surface of the liver, and sometimes a part of the pericardium. The extent of lymph interference then may be reflected upon several membranes as well as the esophagus. It is impossible to check the lymph flow in certain nodes without affecting in some regions several different organs or membranous coverings. The esophagus may be constricted through lesions, and when this condition is present we also find a lymph space obstruction which reacts and makes the altered change more marked. The esophagus passes through the diaphragm and we may find there at times, through costal lesions, an altered flow. In gastroptosis the esophagus is extended sufficiently at time to affect the lymph in the spaces of its mucous and muscular tissues. The absence of nodes within the esophageal tissues throws the burden on the collecting nodes in adjacent areas. The terminal drainage points must receive the most consideration. |
{kind=link}
{kind=link}