
|
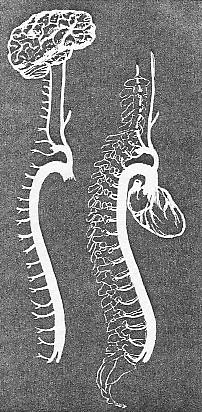
In Relation to Acute Poliomyelitis We have already mentioned that the most direct area of infection in infantile paralysis is through the membranes of the nose and throat. The virus gains entrance during respiration and deglutition. We have also referred to the mode of infection through the alimentary tract. The virus is carried along with the bolus of food and enters the stomach. During the process of digestion it is conveyed to the intestinal tract and the system takes up the virus and its poisons by way of the lacteals and blood channels. A more direct infection of the central nervous system may take place through the lymphatics of the head and neck. The membranes of the nose, nasopharyngeal region and mouth are rich in lymphoid tissue. The close connection between the lymphatic tissues of these areas and those found in the head and neck allow a conveyance of the virus to the membranes of the brain and spinal cord. The openings for communication are numerous and the paths for the conveyance of infection are closely connected. The superficial and deep lymphatic vessels and nodes found in the neck and throat allow of ready communication and transmission of the micro-organisms and their toxic products. The central nervous system may be almost directly invaded by the virus found in the membranes and lymphatics of the nasopharyngeal region. Once the virus reaches membranes protecting the central nervous system the upward invasion to the brain from the cervical region is readily accomplished. The cerebro-spinal fluid surrounding the cord also supplies the area around the brain. There is a communication between the cord and brain, as the same coverings that surround the cord are continuous with those covering the brain. One of the most noticeable symptoms in an acute case of infantile paralysis is headache. There is also pain in the neck. The temperature increases in a typical case until it reaches 103 degrees or more. The congestion in the head and neck is marked. The neck seems swollen; the lymph nodes are enlarged and indurated. The lymphatics are involved as well as the blood vessels. The lymphatics have carried the virus to the hidden membranes of the central nervous system. The invasion may have taken the route found in the cervical region, the cephalic membranes first becoming infected. The virus in this case must needs travel downward in the central nervous system if the case is one that is not abortive in type. General infection of the cord may or may not take place. The cephalic membrane involvement may be sufficient to cause a bulbar paralysis which will eventually affect all points below and prove fatal in nature if sufficient destruction takes place. Again, it is the amount of resistance the tissues have that will determine the extent of the destruction in the nerve cells. The lymphatic engorgement will depend upon the lack of freedom of circulation and the quality of the blood and lymph. The nodules will indurate in proportion to the amount of blockage. The more regular the circulation the better the oxygenation of the blood will be, and good blood, well acrated, is the best of germicides. The microorganisms lose their power in proportion to the vitality of the tissues they have to work in. The extreme amount of congestion in the head and neck is due in part not to the virulence of the virus as much as to the amount of obstruction found in relation to the blood vessels and lymph channels. The involvement of the lymphatics is due in the first place to the more ready infection and conveyance of the virus by the fact that the tissues in which these vessels are found were devitalized by obstructed or impeded circulation. The normal tissues in the pharyngeal and nasal regions of a child will not harbor nor convey to the same extent the virus as in the case of a child in which adenoid growths and diseased tonsils are found. The child with polypi and congested turbinate processes will likewise harbor germs and propagate them in a soil that is suitable for germ development through obstructed lymph and blood channels. The cause of this static condition in the sinuses
of the head and the membranes lining these as well as lining the pharyngeal
region may be due to a variety of lesions. There is always a possibility
of hereditary weakening or diathesis with nervous instability, but we will
discuss here the part the osseous lesions play in the role of primary causative
factors.
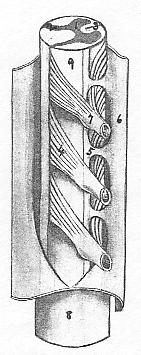
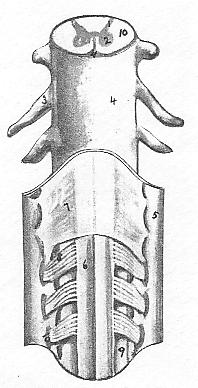
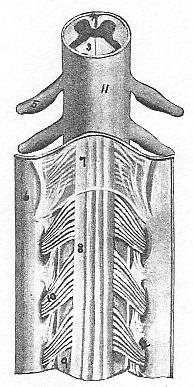
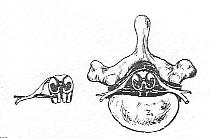
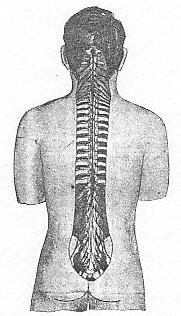
The drainage of the lymphatics of the head and neck is quite the same on both sides. Below the neck and for the rest of the body we find a vastly different proposition. The lymphatics of both sides of the head and neck tend to pass downward to a common collecting centre, the subclavian veins. The superficial communicate in some instances with those of the opposite side. Normally the nodes are not over-sensitive unless pressed upon. Induration is pathological if found to any extent. The same rule that governs the freedom of circulation of blood is more or less applicable to that of the lymph channels. Lesions that contract muscular tissue will obstruct lymph channels the same as they will obstruct the blood vessels. Not all lymphatics have vasomotors supplying them, it is true, but there are other ways of obstructing the flow of lymph and blood than through the vasomotor nerves. The lesions mentioned under the heading of Cervical in the preceding chapter are applicable to lymph channels as well as to the blood vessels. The lesions that produce a congested condition of the tonsils will invariably affect the lymphatics that are so abundant in this region. The lymphatic tissues that form the outer and inner defences of the naso-pharyngeal region suffer obstruction and nodular enlargement whenever there is venous stasis. The involvement of the membranes of the sinuses of the head are either secondarily or simultaneously affected through a vascular disturbance in the vault of the pharynx and the region of the nose. The congestion in the membranes protecting the central nervous system are the effects of lymph and blood vessel obstruction through a lesion of some nature -- osseous or otherwise. Before congestion there must be obstruction, and before invasion and toxic poisoning from virus there must be a suitable soil or else the tissues would produce an abortive condition. Thus we see first, last and always the greatest preventataive measure in infection of any nature will be the maintenance of normal circulation both in the lymph channels and in the blood vessels. This accounts for the numerous cases of the abortive type of infantile paralysis, and also the noted fact that in many instances only one or possibly two in a family of several children contract the contagion; the others not becoming infected. Fortunately, the microorganism of infantile paralysis does not attack children as numerically as the germs that are connected with some of the other and more common diseases. In scarlet fever, measles, whooping cough, etc., there seems to be a condition that makes the contagion spread with a more decided virulence. It is not uncommon to see these childrens diseases go right through the family. PLATE IX. The lymph spaces found in the membranes of the cord are numerous. Right lateral view of cord and the formation of spinal nerves. The lymph bathing the cord and spinal nerves is found in abundance. -- (1) Anterior horn. (2) Posterior horn. (3) Anterior median fissure. (4) Posterior spinal nerve roots. (5) Ligamentum denticulatum. (6 & 8) Dura mater. (7) Posterior ganglion. PLATE X. Anterior view of the cord and membranes. The lymph bathes all these cells and tissues. (1) Posterior horn. (2) Anterior horn, (3) Spinal nerve with covering. (4) Dura matter. (5) Turned back. (6) Spinal cord bared. (7) Arachnoid. (8) Anterior nerve roots. (10) (Top number) Lateral surface of cord. (10) Anterior nerve passing through dura mater. In infantile paralysis the central nervous system is directly involved, and the child who, due to lowered tissue resistance from spinal lesions and other conditions, furnishes the most suitable tissue soil, is the one that will be the victim. The others may have the germs in their mucous membranes, but the soil is not favorable to infection and they will have simply an abortive type or will not be affected in the least. The obstruction of the lymphatics may be due to a secondary condition. The presence of stasis in the region of the tonsils may he somewhat chronic in nature. There may be repeated attacks of tonsillitis which may last only a day or two. The disturbance may be almost wholly vascular. Should the obstruction persist and the lymph nodes become enlarged there will be a lymphatic involvement that will tend to complicate matters. Infection will be a natural sequence. The correction of an atlas or axis lesion that will remove any disturbance to the superior cervical ganglion with its postganglionic fibres that control the vasomotors to that region where stasis has been present will reestablish normal lymph flow. Lymphatic involvement may be secondary to a vasomotor disturbance to the blood vessels in the same region when congestion exists. The hyoid bone slightly misplaced will put tension upon one set of the muscles attached to it and cause not only venous stasis but a blocking of the lymph channels, and as a result we will note nodular enlargement in the lymphatic chains. The enlargement of the nodes in the region of the mastoid may be due to an obstruction of the lymphatic channels in the region of the clavicle. The backward luxation of the clavicle with a subluxated first rib may obstruct the drainage of the lymph into the subclavian veins. The middle cervical ganglion may be involved and we may have a thyroid disturbance as well as cardiac irregularity through a cervical lesion. This may in turn cause pressure by thyroid enlargement upon the lymph channels and produce toxic poisoning of the membranes and tissues in the throat, head and central nervous system. The presence of an aneurysm may, through mechanical pressure, cause a greater disturbance than any single osseous lesion. A cervical rib may cause irritation of the brachial plexus and the sympathetic system that will not be relieved until surgical measures are used. Not all disturbances are from osseous lesions in the way of vertebral rotation or subluxations, and not all disturbances are from local interferences. The lymph channels may be affected and infected through disorders in the axillary and mammary region, or even lower down. There is a communication between the lymph channels of the thorax and cervical region back of the clavicles. That is why no diagnosis is complete that does not include a complete systemic survey in each instance. The high temperature of a child or an adult may be lowered by a single adjustment in the upper thoracic, or a similar effect may be brought about through the correction of a cervical lesion. The idea is to determine the exciting cause, if from a lesion, and correct the irregularity if it is at all possible to do so. PLATE XI. Posterior
view of spinal cord. The lymph blocked in acute poliomyelitis prevents
the nerve and cord cells from functioning properly.
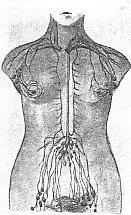
Lymphathics of the Thorax and Abdomen Infection almost invariably complicates the lymphatic system. We are prone to think only of the veins conveying impure blood and producing congestion and stasis, but we must remember always that the lymph channels are the conveyors of toxic products, and blockage in a node or number of nodes will affect the elimination or retard the disemination of toxic products. There is a possibility of the virus found in infantile paralysis cases entering through the bronchial tubes and infecting the tissues in relation to the roots of the lungs. Dust particles include germs, and their entrance via the bronchioles may cause infection and enlargement of the lymph nodes in that area. There is a possibility of the virus or microorganisms of infantile paralysis lodging and becoming scattered through the lymphatics in the thoracic region in relation to the bronchial terminations. Around the cord the pia mater and arachnoid harbor lymph space. These spaces are in communication with the vessels, and it is through them infection enters the cord substance. In the abdomen below the diaphragm the cisterni chyli is located. Into this receptum the intestinal lymphatic drainage enters and the beginning of the thoracic duct is found. This duct collects from the abdominal viscera and passes through the diaphragm in relation to the aorta. The lacteals carry away some of the chyle absorbed from the small intestines and convey the substance to the thoracic duct that passes upwards to empty into the subclavian vein on the left side. The peritoneum is a lymphatic sac in one respect. The amount of absorption that takes place in the peritoneum is great. The food taken into the stomach containing the microorganisms of infantile paralysis are readily absorbed by the lymph channels and conveyed to the blood circulation. The possibilities of mixed infection is worthy of consideration. If a lymph channel is already infected by other germs, it is in no condition to combat the virus of infantile paralysis should it be absorbed. The lymphatic system is in danger of blockage and sluggishness the same as the vascular system. The normality of the nodes and channels of the lymphatic system will depend to a great extent upon the condition of the blood vessels and the tone of their walls. If we find stasis in the mesenteric blood vessels we are likely to find nodular enlargement of the lymphatic system. The numerous nodes found in the mesentery and along the vessels of the bowels are normal only so long as the blood stream to and from the abdominal viscera is normal. A diseased organ is one that has a disturbed circulation regardless of the cause. If an organ is functioning abnormally we invariably find its vascular supply disturbed. If an organ is mechanically interfered with we also find the circulation to that organ affected. The cause being removed the circulation may once more be re-established. The infection of an organ is through its vasacular channels, either the blood or the lymph. The better the circulation the less chance of germ invasion. The more perfect the assimilative mechanism the less liable the virus to be disseminated and propagated. Lymph spaces are found around the cord in all regions. The vascularization of the cord is complete at every segment. The entrance of germs at any point is possible. The normality of the lymph spaces in relation to the pia mater will depend to a great extent upon the normality of the vascular system in relation to the cord and its membranes. If there exist lesions at any point along the length of the cord we at once find a lowered tissue resistance to that area of the cord. PLATE XII. Vascularization of a section of the spinal cord, showing the three spinal arteries and correlating spinal branches from the intercostal. The cerebro-spinal fluid is of a lymph formation, and the area is bathed by this fluid also. There may be a trophic disturbance or a vasomotor instability to the vessel walls, or we may find stasis from a contractured musculature that will block the lymph spaces. In any of these conditions the tissue vitality will be undermined and invasion is more apt to take place. In the thoracic region we may find costal lesions as well as vertebral. The relation of the intercostal vessels to the ribs may, in a costal subluxation, so disturb the sympathetic ganglia that the tissues around the foramina will become irritated, and this will extend into the cord through the blood channels. The blockage of one vessel to the cord and membranes may so lower the nerve and cell integrity that a cord segment will become readily infected by the virus. Remember that the cord segments and their cells must be kept at a certain tone from a vascular standpoint or else the cells will not function normally. In the ventral portion of the grey matter of the cord the motor cells send forth their efferent impulses, and the muscular tone of the limbs will depend upon the normality of these impulses for their strength and motion. The lowered tone through disturbed vascularization, plus the invasion of the virus or its toxins, even in a mild or abortive case, will cause a disturbance to the efferent tracts in proportion to the degree in which the cells resist the attack. In the more severe cases of infantile paralysis, where exudation accompanies congestion, we note a marked destruction of the motor area. If the spinal arteries and veins are obstructed to any extent the lymph spaces are occluded, and natures effort to clear the condition is sorely handicapped. Thus we see the prime importance of keeping a childs spinal tissues up to normal so that should the virus gain entrance to the body there will not be lowered tissue resistance in the region of the central nervous system. The region of the diaphragm, with its many openings for the passing of nerves, vessels, tubes, etc., is of interest. The presence of lower rib lesions or vertebral misplacements may so affect the attachments of the diaphragm and its crura that the openings found in its central tendon and in the region in relation to the vertebral column may cause undue pressure or obstruction to these various tubes, vessels and nerves. PLATE XIII. General Scheme of Lymphatics. The veins and thoracic duct are passing upward; the nerves, aorta and esophagus are going downward. All have their functions and any minor obstruction may cause a systemic disturbance. The thoracic duct has a few valves to prevent backward flow. It is a long tube, and gravity is against it the same as in the saphenous veins. This duct has its vascular supply and nerve tone, although it has not the marked muscular tissue within its walls that is found in the blood vessel walls. The thoracic duct is a great collecting system and the flow of lymph must be emptied into the veins as regularly as possible. From the fact that the lymphatic system has to deal with toxic products, we must at all times determine the condition of this duct and see that no lesion exists that will in any way affect its walls or its conveying properties. The cisterni chyli is located in front of the second and third lumbar vertebrae. Lesions that are found at this region, or even higher, including lower costal, may have a marked effect upon the receptive properties of this collecting system. The drainage of the mesenteric nodes into this cistern
will depend upon the normality of the blood vessel circulation. The
presence of obstipation, with poor peristaltic action, the finding of adhesions
or the noting of growths and thickening of the tissues, all have a bearing
upon the lymphatic system. Splanchnoptosic conditions will affect
drainage and obstruct the lymph channels. This will lower the general
tone of the tissues. In children colic, convulsions and constipation
will lower the vitality.
The common point of tissue irritability is when we find a lesion from a fall or strain. The disturbance to the vessels and nerves, unless the proper adjustment is made, will continue to lower tissue resistance through nerve irritation. If the sympathetic chain is involved through its connection with the spinal nerves, the vasomotors will suffer from impeded circulation, and the impulses will become irregular. The spine of a child from the time it is born must be inspected if we wish to keep him free from lesions and scoliosis. Some children grow up with amost perfectly aligned spines, while others, through traumatism, suffer irregularities that adjustment alone will rectify. PLATE XV. The spinal cord and nerves exposed. The lymph bathes the entire tract. |
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}