
|
General Statement The arrangement of the lymphatics in the neck are such that there is every possibility of a checking or blocking of the lymph flow through lesioned vertebrae or muscular tension. There is also the fact that the blockage of lymph nodes or vessels in the neck produces hyperplasia of the lymph tissues in the head. The deeper neck glands may be enlarged for a time quite distinct from the enlargement of the more superficial glands. While the superficial and deep glands are closely connected, and their drainage point remains the same, yet through throat infections or cervical lesions the one set may become involved before the other is affected. The relation of the nodes to the nerves and blood vessels is significant. If sufficiently enlarged they may produce pressure sufficient to create undue stimulation on nerves passing through the neck, resulting in accelerated heart action or bronchial and gastric irritation. This may be a new application or viewpoint, but may be demonstrated in the clinic room. The enlargement of nodules may interfere with salivary secretions through pressure and cause a dry mouth or lack of saliva. Enlarged glands may block the capillaries and veins and produce a flushed face. This point may be demonstrated when the patient has a cold and the glands in the neck and under the rami of the inferior maxillary are enlarged. In the chapters written by the specialists on eye, ear, nose and throat, you will find more detailed statements regarding these points. In this chapter we outline in a general way the possibilities of interference and blockage through lesions in the same respect as we treat lymph flow interference in the chapters dealing with the rest of the body. We want to make it plain that in order to correct
any disturbance in the head we must look well to lymph drainage at every
point where there is a possibility of obstruction.
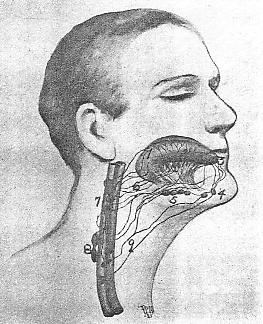
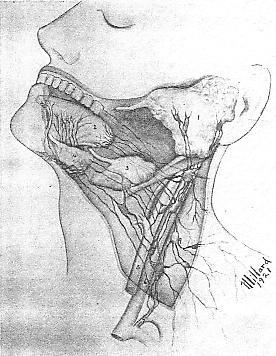
Lymphatics of the Tongue The tongue has more nerves, vessels, lymphatics, and variety of functions than any organ of its size in the body. The lymphatic drainage of the tongue includes vessels and nodes that carry away the lymph individually and collectively. As in the innervation the tongue seems to be divided into sections, so in the lymph vessels the drainage is quite distinct and separate, yet all channels lead to the deep cervical glands in the region of the beginning of the two carotid branches from the common arterial trunk. The submaxillary lymph nodes collect lymph from the free end of the tongue. The deep cervical nodes collect from the nodes on the hypoglossus muscle. These later lymph channels follow the ranine vein. Beneath the epithelium of the tongue, the lymphatics have their beginning. In the base of the tongue the lymph vessels connect freely, while in the free portion there is quite a distinct individual drainage. There are small lymph vessels originating in the muscle of the tongue, but the submucous vessels are in the vast majority. This lymph network is so arranged that the vessels are readily drained unless there is blockage in the nodes, especially in the submaxillary region. The submental lymph glands receive a part of the drainage. Small lymph vessels from the tip of the tongue perforate the mylohyoid muscle in some instances, and end in the node above the hyoid. The lymph nodes just above the omohyoid receive some lymph vessels. The relation of these lymph vessels to the hyoid bone and the digastric muscle is of significance. Lesions affecting the position of the hyoid bone may interfere with the drainage of the lymph, while lesions disturbing the innervation of the digastric muscles may also cause lymph blockage. This applies also to the mylohyoid muscle referred to above. You will notice by Figure 2 that the drainage from
the apex of the tongue ends in nodes much lower than does that from the
base of the tongue. Where the digastric muscle passes in close proximity
to the jugular vein, there are nodes receiving considerable drainage.
The contraction of this muscle unduly causes blockage in the nodes and
lymph vessels. There is also a large node at the point of crossing
over of the hyoid omohyoid at the jugular vein: the inferior node of internal
jugular. Lesions affecting the innervation of this muscle or subluxation
of the hyoid, may cause retardation of lymph flow. The superior deep
cervical nodes collect lymph from many lymph vessels and their obstruction
through blockage in the thyroid gland region must be carefully noted.
The drainage from the tonsillar region is closely connected with that of
the drainage from the back of the tongue. This will account for enlargement
of certain nodes when a cold or sore throat is found.
As stated above, the nerves to the tongue are unusually
numerous, and the vasomotor supply through the sympathetics controlling
the lingual blood vessels is a point not to be overlooked. The lingual
veins are readily interfered with at certain points and if stasis or edema
exists there will be interference with the lymph flow.
Treatment To regulate the vasomotor control of the blood vessels in the tongue, we must first of all see that the muscles of the tongue are not disturbed through lesions that affect the innervation of these muscles. Any cervical lesion, or even upper thoracic, may cause a vasomotor instability. The hyoid bone may be slightly or markedly out of alignment through traumatism or extreme lateral muscular tension. Lesions affecting the scaleni muscles may cause costal traction of the first or second ribs and produce a blockage of the lymph at or near the terminals of the lymph vessels. The slightest amount of blockage in the lymph nodes and vessels will back up or check the drainage from some portion of the tongue. The arrangement of the lymphatic vessels from the tongue is unique in that there are so many separate channels and distinct areas drained through different sets of nodes. The vessels from the anterior part of the tongue pass through different sets of nodes than do those from the basal part. Eventually, they collect in the cervical nodes that convey the lymph to a common terminal in the veins on either side. The lymph vessels from the tongue pass or pierce muscles continuously, and any tension on these muscles, or any enlargement of the salivary glands, will cause more or less blockage. The tongue possesses such unusually good blood and lymph drainage, and from the fact that it is such a movable organ, we find very little trouble or disease, especially of a malignant nature. There is, however, a possibility of one or more of the nerves becoming lax in their tone and causing symptoms so well known to all physicians. The condition of the deep cervical lymph nodes is
the most important consideration, as the numerous lymph vessels from the
tongue to these deep centers are so varied that blockage is not likely
to occur sufficiently to prevent a marked checking in the drainage until
the deep glands are reached. If they are blocked, there will be a
checking of the lymph streams in the numerous vessels entering the deep
nodes.
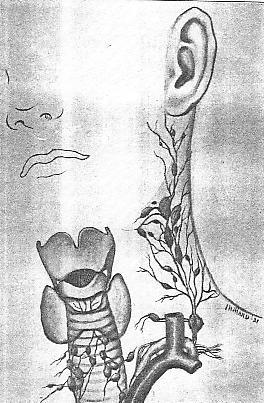
Lymphatics of the Thyroid Region In order to understand clearly the drainage of the lymphatic system of the neck and head, we will begin with the thyroid gland and discuss the lymphatic drainage in this the lowest region. The prevelance of goitre in certain districts has never as yet been clearly explained. There are many theories and it does seem in many instances that drinking water has an influence upon this gland in a chemical way. The different kinds of goitre that are found tend to complicate matters, as there has been no explanation, satisfactorily given, as yet, as to why one person should have exophthalmic goitre and another person a cystic goitre. Anatomically, we know that the thyroid gland contains many lymphatic vessels and that they are often large in size. These lymph vessels must have drainage finally into the lymphatic ducts at the junction of the jugular and subclavian veins. The thyroid arteries, the superior and inferior, supply the bland and receive vasomotor fibers from the cervical symphathetics. The relation of the arteries to the various structures in the neck are such that there is usually little interference from muscular tension, but there may exist cervical lesions that cause undue disturbance of the innervation to the vessels in the gland. We are undecided as to the vasomotor control, directly or indirectly, of the lymphatic vessels and glands in and around the thyroid, but we believe, from clinical evidence, that these lymphatic vessels are influenced, indirectlly at least, through the middle and inferior cervical sympathetics. Cervical treatment, including springing of the vertebrae that influence the middle and inferior cervical sympathetics, will oft times reduce some types of goitre without any manipulation directly over or around the thyroid gland. This would seem to indicate that while the vasomotors of the thyroid blood vessels are directly controlled, the lymphatics as well are at least indirectly reached. It would be quite impossible to reduce an enlarged thyroid gland by controlling the vascular system only if there existed lymph blockage that was causing a portion of the enlargement. In goitre cases there is interference of the drainage in the right lymphatic duct, as well as the thoracic duct at their points of emptying. This may be verified by the edema that is so often noticed above the clavicles and laterally to the thyroid gland. Further proof is found in the enlarged cervical nodes above the gland through blockage or lack of proper drainage of lymph into the veins. The nodes located at the termination of the common carotids collect part of the lymph from the thyroid. There is also a node or two anterior to the larynx just above the thyroid gland that collects a portion of the lymph. In front of the trachea there are a few nodes that collect from downward coursing lymph vessels. The recurrent laryngeal nerve lies in the path of a small number of nodes that collect from the sides of the thyroid gland. In certain cases of laryngeal cough and laryngitis we have found that these nodes seemed, when enlarged, to press and irritate the nerves, and when reduced, and the lymph vessels drained, the cough subsided. There is no doubt in my mind but what indurated or even enlarged nodes, not hardened, cause a great deal of disturbance to nerves in the course of these nodes. We will discuss later the effects of the deep cervical or internal jugular nodes in their relation to the pneumogastric nerves and brachial plexus. PLATE III. Lymphatic drainage of the Thyroid Gland and Larynx; also the thoracic duct receiving the lymph from the cervical nodes. The deep cervical nodes and channels above the thyroid
collect and conduct downward the lymph that clears the vessels in the thyroid
gland. In some instances it would seem that goitre was a lymphatic
disturbance. If, for any reason, the thoracic and right lymphatic
ducts are blocked at their terminals there must be a checking also of the
drainage of the lymph vessels in the thyroid gland. The lymph vessels
are numerous in the gland and their drainage course is in two directions
at least, an upward, or ascending, and a downward or descending.
Then there is the additional lateral drainage. Disturbed innervaation
to the thyroid gland and blood vessels must have a bearing also upon the
lymphatics in the thyroid. This may acount to a poisoning of the
substance of the thyroid that would tend to increase its size. Draining
of the lymph vessels certainly reduces the size of the goitre.
The lesion theory is very applicable in this instance. Drinking water, nervousness, or other influences may have caused the thyroid to enlarge, but in every instance where goitre is present we have found one or more osseous lesions that had a bearing upon the case. Usually there are upper thoracic lesions with a corresponding interference with the great vasomotor centre at the first and second thoracic. It is at this centre that the circulation of the blood cephalad is controlled. The nerve fibres pass through the inferior and middle cervical ganglia on their way to the superior. As stated above, the nerve supply of the thyroid may be found in the middle and inferior ganglia. Thus we see how the drainage of the vessels in the thyroid may be influenced by upper thoracic lesions. Venous stasis always interferes with lymphatic drainage. Vasomotor changes may indirectly, through venous stasis or edema, influence and retard lymph flow. Indirectly then, in any case of vascular irregularity, the lymph stream is affected. The upper costal attachments must be noted to determine
any costovertebral subluxation, and the clavicles must articulate properly
if we are to expect free drainage in the lymph ducts. The venous
drainage of the thyroid terminates almost at the same point as the lymph
drainage, and the innervation of the thyroid corresponds with the centres
for its vasomotor control.
Likewise, the blockage of the deep cervical chain of glands through any of the various disturbances found in the head and throat may interfere with the reduction of a goitrous condition. We see more and more the necessity of keeping the lymph flow cleared in any region where there is swelling or congestion, adjacent or remote. First of all, in any instance, the terminals of the lymph tubes must be kept free from any interference or obstruction; second, the specific control of the vasomotors to enable the calibre of the vessels to respond to normal impulses; and third, the adjustment of all lesions to insure normal tone and regulation of nerves and vessels. It is in this same region, that of the middle and interior cervical ganglia, that we partially influence heart action, and these cardiac nerves are often interfered with by venous stasis and lymphatic blockage through enlarged nodules and an edematous condition of the tissues. Tachycardia, so pronounced in exophthalmic goitre, may be influenced through a disordered lymph system. The close relation of the lymph in cell spaces, or pericellular areas, may in lymph blockage, have an irritating effect upon the cardiac nerves from the cervical sympathetics. We will discuss later the ophthalmic phase in goitre, and demonstrate the bearing the lymph nodes and vessels have in their relation to those in the parotid and upper cervical regions. The blockage of the lymph in goitre cases has a direct bearing upon the drainage of all the lymph vessels and nodes above the thyroid. This explains the peculiar symptoms noted in the organs of the head, as well as in the throat, when goitre exists. The interference of lymph flow at any place between the duct terminals and a remote area invariably means a series of lymph disturbances at the points beyond the blockage. We have tried thus far to show the advantage of considering
the thyroid region as a strategic point in the drainage plan of the lymphatic
vessels in relation to points above. We will now take up the region
of the larynx and show how necessary free drainage of this area is, to
clear the lymph vessels and nodes above.
As stated on the preceding page, the drainage of all nodes and vessels above must necessarily pass by the region of the thyroid to drain into the subclavian vein. The freedom of blockage to the lymphatic vessels in the larynx will depend on the free flow of lymph below this region. As in the thyroid body, there are two sets of laryngeal lymph vessels, the superior and inferior. Their drainage course, after passing through the thyrohyoid and cricothyroid membranes, is outward and downward toward the deep cervical glands. The inferior sometimes terminates in the node lying in front of the cricothyroid membrane, or in nodes in front of the trachea in relation to the inferior thyroid artery. These nodes, sometimes referred to as the anterior cervical nodes, lie in front of the larynx and trachea, near the anterior jugular vein. The deeper set drain the lower portion of the larynx and the upper part of the trachea. This last set also drain the upper part of the thyroid gland as already pointed out. The main collecting nodes for the lymph of the laryngeal region are located at the bifurcation of the common carotid and on the inferior thyroid artery. These deep cervical nodes lie in the course of the terminal drainage of the lymph stream from the head and neck. Some of the lymph vessels follow the superior laryngeal
artery. The larynx with itds vocal cords is controlled and innervated
by the superior and inferior laryngeal nerves. The sympathetic nerve
filaments follow the laryngeal nerves. Control of the cords and action
of the various muscles attached to the vocal box are dependent upon normal
nerve impulses. The vascular supply is controlled through the sympathetics.
The venous and lymph drainage insures a clearance of these various muscles
and tissues.
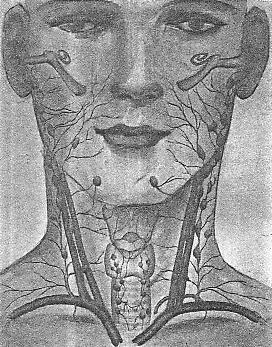
Treatment The tone of the nerves depends upon the freedom from pressure or irritation at any point along their course. If cervical lesions exist, causing muscle contraction or stress upon nerves and tissues, the tone of the laryngeal muscles will be lowered. If there is vasomotor interference in any way, there will be corresponding irregularity in the supply and drainage in the larynx. Vascular insufficiency will mean lymphatic disturbance and a checked flow of lymph. Congestion of the laryngeal membranes or tension of the laryngeal muscles affects the lymph flow and this condition will remain until normal tone is re-established through the correction of lesions and the relaxation of the muscles under the jaw in the region of the hyoid. Blockage of the lymph stream at a lower point in the lymph vessels or nodes, will cause interference in the laryngeal region. This will explain why we considered the thyroid gland region first. There must be an outlet for the lymph in order that the laryngeal region may clear itself. Each nerve and vessel going to the larynx must be insured normal freedom. Any lesion that will interfere with the laryngeal nerves will cause disturbance according to the functions of that nerve. The recurrent laryngeals, with their peculiar loopings, may be interfered with by nodular enlargements or thyroid swelling, or lesions that have tensed the muscles over the course of the nerves. The vasomotors that regulate the laryngeal arteries indirectly, if not directly, regulate the lymph vessels, either at the drainage points in the larynx or in the larger vessels that receive and carry onward the flow of lymph. Here, again, we understand the cardinal point in every disease, namely, due consideration of the drainage at every point between the affected part and the termination of the stream. The deep cervical lymph nodes collect eventually the lymph of the head and neck, and it is well to trace the nodes as nearly as possible and see that there is no undue enlargement or blockage of lymph. There are many lesions that may cause nodular enlargement, outside of toxins which overtax the nodes. We will consider next the lymph drainage of the tonsils. We do this before discussing the drainage of the gums because we want to emphasize certain glands and nodes that have a bearing upon the lymph vessels. The drainage of the upper part of the trachea is often different in its termination than the lower part. The upper part is drained in common with the thyroid gland region, while the lower trachea is drained in common through the tracheo-bronchial nodes which eventually unite with the broncho-mediastinal trunk that may empty at a different point in the subclavian vein than does the right lymphatic duct, or even the thoracic duct. There may be a blockage of the upper tracheal nodes and yet the lower tracheal nodes may have a free lymph flow into the vein. PLATE IV. General scheme
of lymph drainage of head and thyroid regions.
Lymphatics of the Tonsils Under this heading we wish to discuss the general lymphatic drainage of the naso-pharyngeal region. This general discussion will include the various lymph glands and adenoid tissues. We will leave the applied anatomy of the eye, ear, nose and throat to those who have written upon that subject. Our intention is to call the students attention to the drainage, in a general way, of an area so closely studded with lymphoid tissue. It will be necessary to include drainage points and receiving nodes that exist in the region of the mandible. In this general drainage we will note the possibility of interference in several places where muscles may, through undue tension, block the lymph flow. We will also refer to the location of the salivary glands and show that the effect of enlargement may interfere with the drainage of the lymph flowing from points above. If all of the lymph vessels and nodes of the tonsillar region could be shown along with all receiving and collecting nodes, also efferent lymph vessels, we would observe that rings within rings of lymph vessels, including nodes, would complete the circles. One circle would not include these vessels and nodes, as described by some authors. Three or more distinct rings may be noticed. The first would include the palatine tonsils, the lingual nodes, and lymph vessels. Outside of this ring a second would include the pharyngeal tonsil, the Eustachian tonsils, retropharyngeal glands, styloid, and lateral pharyngeal glands. The third ring would include the nodes found on the sternhyoid muscle and at the termination of the common carotid artery; also a node or two on sternomastoid. In front under the mandible, the submaxillary and submental nodes, and finally the hyoid nodes. These three circles will make clear the lymphatic drainage of a region so rich in lymphoid tissue. First, we will show the drainage of the inner ring. The tonsils are drained by lymph vessels that pierce the walls of the pharynx on their lateral surfaces and end in glands by the walls of the internal jugular veins. The arches, adjacent to the palatine tonsils, are also drained by these vessels. The nodes receiving drainage of the tonsils and arches lie on the jugular vein near the lower border of the digastric muscle. Free drainage of lymph in the region of the tonsils and the glosso-palatine and pharyngo-palatine arches may be blocked by traction of the muscles in this region. The nerves supplying the muscles may, through lesions, be contractured, or congestion of adjacent parts may cause undue stress upon the tissues. The digastric muscle may have disturbed innervation and cause the muscle to draw upon the lymph vessels leading to the nodes on the jugular vein. The styloglossus also, if contracted, may interfere with drainage of lymph from the tonsillar area. The vascular arrangement of the tonsils is unusual, as four arteries at least supply each gland. However, all of these arteries are branches of one main artery, the external carotid. It is the venous and lymph drainage of the tonsils that interests us most. If the veins are compressed through congestion, scar tissue, or muscle contraction over or around them, we are more apt to find a retarded flow of lymph. Enlarged nodes at a lower point will back up the lymph and cause a disturbance in the tonsils and adjacent tissues. Again we see the need of a clear lymphatic drainage all the way down to the terminals in the subclavian veins. In tonsillitis the lymph nodes enlarge almost immediately and can be palpated readily near the angle of the mandible. If unduly blocked for a period of time, other nodes enlarge and there is a general edematous condition of the tissues under the ramus. It does not take long to block lymph nodes and vessels and unless they are cleared the nodes in adjacent regions show enlargement. First of all, in tonsillar infection, we must start at the supraclavicular area and establish free lymph flow, then work to clear the nodes above that point. Every muscle should be relaxed through the points of innervation. That is, the correction of lesions that will allow free impulses to the muscles. The lymph stream is readily checked in many ways. The lymph vessels are pliable and readily compressible. Indurated nodes are often found that have been blocked so long through lack of treatment that would have cleared them when they were pliable. Often enlarged nodes in children following colds or some infectious disease are allowed to remain congested and finally become indurated. In these cases, the lymph must follow other vessels that partially lessen the load. It is well to watch the nodes in children and re-establish good lymph drainage. This may save secondary infection at a later date. It is comparatively easy to regulate the lymph stream in a child if taken when the vessels and nodes are first blocked. The most common source of bronchial and lung infection is through the throat; very seldom do we find a tubercular condition that has started from any source but by way of the throat. The blockage of the cervical lymphatic glands will cause enlargement of the bronchial glands and then it is but a simple matter for the nodes at the roots of the lungs to become involved. Infection passes downward readily, unless the lymph vessels and nodes are cleared and properly drained, into the lymph duct and then the subclavian veins. The lingual drainage has been discussed earlier in this chapter. We thus see that the inner circle collects the lymph and passes it through nodes that are connected with the cervical chain. The second ring includes a greater area. The retropharyngeal nodes are separated from the atlas by the major rectus capitis muscle. This is just back of the upper portion of the pharynx. The nodes through their efferents drain into the cervical nodes that lie near the main vessels of the neck. We have mentioned the retropharyngeal nodes first
in this second ring because the collecting lymph vessels are numerous,
and include several lymph areas, as the Eustachian nodes, and nasopharyngeal
region, and the fossae of the nose. Before the lymph reaches the
deep cervical nodes a number of the channels pass through the subparotid
nodes. The soft palate is also drained through the retropharyngeal
nodes. The drainage of this second ring may be interfered with in
several ways. The location of the retropharyngeal nodes is such that
faulty innervation of the rectus muscle may disturb the free lymph flow.
An atlas lesion may alter the drainage directly or through a disturbance
of the tissues from stress or through tissue congestion. These nodes
are very important lymph structures and lie in a position that makes possible
their enlargement or induration through various lesions of the cervical
vertebrae, or hyoid lesions that cause traction upon the muscles of laryngeal
and tracheal areas. Vasomotor disturbances to these parts may cause
an alteration in the tissues covering the nodes. The subparotid nodes
that receive part of the drainage may be disturbed through pressure of
an enlarged parotid.
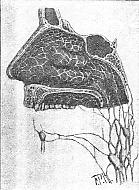
The receiving cervical nodes may already be overburdened with lymph and a backing up of the lymph stream may result in enlargement of the retropharyngeal nodes and a tissue congestion or even hyperplasia result. Cervical muscular contraction, through colds, may produce venous stasis and cause a general blockage in the lymph channels. Lower cervical lesions and even upper thoracic may interfere with drainage at the terminals which will be reflected in the pharyngeal tissues. The third ring and outer one, while more superficial, has a significance in that a vast area is drained. The nodes on the sternohyoid muscle are connected with those of the cervical group chain, also those found on the sternomastoid. This ring includes the submental, submaxillary and hyoid region nodes already referred to. The many lesions that may cause interference with these nodes are readily understood when we notice the areas drained by these lymph tissues and vessels. A subluxated hyoid may cause considerable traction and, on careful palpation, the nodes on one side may be found to be enlarged. The deep cervical may block the more superficial nodes. The mastoid and occipital nodes may be enlarged through the lower interference. It is well to go over all the nodes palpable, and try and determine the relation between the enlarged nodes and the congested areas found upon examination of the nose and throat. The nodes in the three rings are bound to be enlarged more or less when there is pharyngitis, tonsillitis, or Eustachian closure. The nodes will not reduce in size to any appreciable extent until tissue congestion is relieved. We have outlined in a general way the main nodes in these regions. The chapters by specialists on eye, ear, nose, and throat will include more detailed statements. The main point we have tried to emphasize in the lymph drainage of the head is the attention that must be paid to the terminals of the ducts that empty into the subclavian veins. In many cases the fullness of the tissues above the clavicles will be noticed, and that the left supraclavicular area is more likely to become edematous than the right. This fullness must be reduced before we can expect to drain the head lymph vessels. Stasis in the veins will only aggravate the lymph vessels and cause additional blockage in their channels. Vasomotor control of all vessels in the neck and throat will, when regulated, make lymph flow more normal. Indurated nodes may block the lymph stream until collateral circulation is established. It is unwise to work directly over enlarged lymph nodes. It is far better to regulate the blood vessel flow and work to the end of freeing the lymph stream through reducing the general tissue congestion. PLATE VI. Lymphatics
of the mastoid, occipital and cervical regions.
Lymphatics of the Teeth and Gums In discussing this section of the head we might say that texts attach too little significance to the lymph vessels found in the alveolar region. Histologists are prone to pass by the subject of lymph vessels in connection with the teeth and gums, and dental anatomist are equally reticent. Bailey gives credit for Schweitzers statement that an arborization of small lymph vessels in the pulp of the crown, converging to a few larger lymph vessels in the root pulp and accompanying the blood vessels through the foramina of the apex is observed in histological findings. Lymph channels in the pulp are minute but they have a bearing upon the drainage system that insures, when cleared, normal tissue. We are inclined to believe that wherever there are arterioles and capillaries, there are corresponding lymph spaces and capillaries, and that wherever there are capillary veins, there are lymph drainage spaces or channels. The lymphatic drainage system is so complete in the various organs and tissues of the body that we have come to depend upon our treatment of this system to clear any possible congested or disturbed tissue condition. The pulp of a tooth is the life of it, and drainage is always equally important to supply. The gums are well supplied by plexuses of capillaries. On the inner surface of the gums from the mucous membrane the collecting ducts have their beginning. From this point they pass between the teeth to a duct that collects the lymph. The arrangement is of a semicircular plan and lies on the outer surface. The submental nodes receive the lymph from the front lower gums. The submaxillary nodes collect from the back gums both upper and lower. The buccinator nodes sometimes collect a part of the lymph; also the superior deep cervical glands. The lymph vessels of the teeth follow practically the same course. The upper deep cervical nodes eventually collect the lymph. The blockage of lymph in the gums and possibly in the pulp marks the beginning of abscesses and pyorrhoea. Perfect blood supply and venous and lymph drainage will prevent decay, providing tartar is kept cleared and food particles removed from between the teeth. The gums in order to have tone and remain pinkish in color must have proper blood supply and free drainage. Systemic disorders and anemic conditions affect the teeth and we can hardly expect to establish a local tone when a systemic absence of tone exists. Much can be done, however, in keeping the gums healthy if we watch the lymph drainage. The blocking of the submental or submaxillary nodes will shortly cause a disturbance in the gums. Any lesion that will contract the hyoid muscles or laryngeal tissues may interfere with the lymph flow from the gums. The vasomotors to the blood vessels supplying the teeth and gums may be affected by cervical lesions. The veins and lymph vessels will be affected by muscle contraction causing blockage of nodes in the deep cervical group of glands. The presence of goitre may affect the gums and teeth through a checking of the venous and lymph vessel flow. Subluxations of the mandible or hyoid will cause, in some instances, enlargement of the salivary glands and block lymph flow. The muscles attached to the mandible are often contracted through lesions and this will interfere with drainage. In order to have perfect circulation in the teeth
and gums, we must not only keep them cleansed, but see that no interference
with the supply and drainage exists. Too little stress has been laid
upon the lymph drainage of the gums and teeth.
PLATE VII. Nodes in
Relation to Salivary Glands -- (1) Parotid gland (2) Tongue. (3)
Submaxillary gland and lymph node. (4) Sublingual gland and nodes
adjacent. (5) Carotid artery. (6) Internal jugular. (7)
Thoracic duct. (8) Node receiving lymph from the tongue and
parotid region. (9) Deep cervical nodes. (10) Submental node.
(11) Lymph drainage from gums.
Pyorrhea Lymphatically Considered Until recently we suspected unbrushed teeth to be a factor in the cause of pyorrhea. Food particles remaining between the teeth were supposed to cause, or set up, a fermentation that resulted in pyorrhea. On second thought we have changed our minds, because the very people who do not take particular pains with cleansing their teeth oftimes have good teeth. Before tooth brushes were a common toilet article, pyorrhea was not known to exist in the same degree as at the present time. Now-a-days pyorrhea starts with some people by the time they are in their twenties, and sometimes earlier, and at forty dentists find it uncommon not to detect some degree of this trouble. We have labored long to find the cause of pyorrhea, and have recently satisfied ourselves that the cause is clear to those who will go into the subject thoroughly. It is not a germ disease; decidedly, no. It is not necessarily a result of unbrushed teeth conditions, but it is a result of an acrid formation beginning at the extreme root ends of the teeth in the way of tiny abscesses with a granular pus collection. These small abscesses are beyond the reach of the probe, and the root canal leading to a closed cavity in the crown of the teeth prevents this acrid pus-like formation from passing up into the pulp in any appreciable quantity. Instead of following the vessels into the pulp, the acrid accumulation gradually works its way up between the gums and the roots of the teeth and loosens the gums from the teeth. This acrid fluid substance affects the gums to the extent of causing them to recede and the peculiar odor and color of the gums verify the statement that the pyorrhea collection of acrid pus is destroying the gums and causing an alveolar disturbance that leads to but one thing: extraction. Now, we will go back to the primary cause of pyorrhea and lead up to the acumulation referred to above. The beginning is a combination of liver and kidney trouble, and back of this disturbed organic condition is a faulty circulation and innervation of these organs. The chemical changes in the lymph stream and nodes due to altered function of the liver and kidneys reflect themselves in time upon the salivary glands and adjacent lymph nodes. It resembles a mild uraemic poisoning. The altered salivary secretion, the lymph node enlargement and changed lymph substance, both combine to produce in the vessels and lymph spaces around and to the teeth, a substance acrid in nature. Through liver and kidney alterations in function and secretions, a deposit of toxic products causes destruction of tissue at the extreme points of the teeth rooth resulting in tiny abscesses. This may be unlike an alveolar abscess in that the changed lymph substance combined with the salivary gland secretion may be more acrid and of a more destructive nature. When this acrid pus formation starts to eat its way toward the free gum surface there is an odor given off which is not hard to recognize. The lymph vessels between the teeth convey this eating fluid to adjacent teeth roots and soon three or more roots are involved. There are certain fluids the specialists use to counteract this pyorrhea condition, but it is difficult to reach because the tip end of the roots contain the first trace of acrid pus. The lymph nodes in any case of pyorrhea are invariably affected. The poisons are retained and tissues are being eaten away. The salivary glands no longer secrete a normal substance, as there is lymph blockage and accumulated poisons in the way of toxic products from a systemic disturbance caused by an altered organic change in the liver and kidneys. Thus we find the cure of pyorrhea is one of prevention. The liver must be kept functioning normally and the kidneys performing a normal secretion of fluid. Lesions that cause a lack of regularity in the blood supply to the kidneys and liver, or lesions that cause lack of nerve tone or vasomotor control will be the primary cause of pyorrhea. We are living in a different age and under different circumstances than did the people of a generation or two ago. We have nerves now-a-days, and we have changed secretions in the various organs. The influenza epidemic is an example of what excitement and peculiar weather conditions may bring upon a people who live constantly on high tension. No organ can function normally when the mind is constantly agitated, and excitement prevails. The cause of an increase in pyorrhea is due then not only to lesions of an osseous nature, but lesions of a mental nature as well. We consume in our nervous state chocolates and finely ground food stuffs, and we wonder why our teeth go bad. We go along with a slight blood pressure or a mild nephritis and still expect that a systemic distubance will not reflect itself upon some weakened tissue. Changed chemistry in the lymph vessels and nodes along with altered secretions of the glands in various regions will result in pyorrhea as well as weak eyes, and general symptoms that are always associated with these altered states of the body mechanism. In this connection we might add that the gastric disorders found in connection with the diseased teeth is but a secondary poisoning through salivary secretions being carried downward from the mouth in swallowing. If the pyorrhea is adanced, the additional exudate from between the gums and roots of teeth will mix with the salivary secretion, and result in gastric disorders. We never find pyorrhea affecting the teeth and gums alone. There is always an additional poisoning of the various weakened areas of the body by the lymph stream that is overladen with toxic substances from deranged organs. In some cases the whole system is affected; joints, muscles, and various tissues. The peculiar localization of pus at the roots of the teeth is due to the combination of lymph and salivary fluid concentrating upon a fairly closed cavity that is more or less liable to the collection of saliva and to tartar formations. There is no other proposition in the human body quite like that of the alveolar sockets. The peculiar pressure upon the teeth in trituration and in nervous troubles where there is a grinding of the teeth, make the sockets containing the roots of the teeth liable to irritation if there is not a normal lymph and blood suppy. As soon as there is an alteration in the blood or lymph the tendency of the gum to cleave is made manifest, and then the combined altered saliva, along with food particles, and the altered lymph make the changes that produce the tiny abscesses, and the eating away of the gums that eventually recede. It is an acrid proposition resulting from an altered lymph flow that has concentrated upon these all-but-hidden sockets or pockets. |
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}