
|
In the study of the lymph drainage of the eye, ear, nose and throat we are opening one of the most fascinating chapters of Osteopathy, a subject of which our knowledge is still so limited that it is as but a minute scratch upon the veneer. The first productive stimulus to this subject was created by the theory of fermentation of the lymph in the lymphatics as propounded by the Old Doctor (Dr. A. T. Still) and subsequently developed by Dr. F. P. Millard. In the early days of Osteopathy the Old Doctor expressed the opinion that each lymphatic created a specific substance, which is discharged into the blood, and that these substances are necessary to the integrity of the organism. The frequent references to the humors and refluxes of early writers indicate that they had a preconceived notion of the lymphatics, the nature and source of which were at that time bound up in apparently unfathomable mystery. It is to the physiological chemist that we must look for the development of our knowledge of this most intricate subject. The gross and histological anatomy as well as the pathology of the structural elements of the lymphatic system have been quite thoroughly investigated, but there is still a vast amount of work to be done in isolating and determining the remarkable properties of the active principles of the lymph drainage. The clinical progress of the subject has within past years, and particularly of late, made rapid strides forward, and an ever-increasing interest and enthusiasm stimulated in those who have become initiated in this most fascinating phase of clinical study. The subject matter of this chapter is, in brief,
a repetition of what I have previously expressed as clinical observations,
which have been so forcibly verified by personal clinical experience as
to create an interest in a subject which solves many of the innumerable
problems incident to the practice of Osteopathy. It is my purpose
to limit my remarks to the important relationship existing between the
lymphatics of the eye, ear, nose and throat, and the diseases treated by
the osteopathic ophthalmologist and otolaryngologist. An understanding
of this phase of physiology, in its normal and abnormal reactions, is of
paramount importance, and serves an incalculable aid in the analysis and
treatment of the upper orifices.
They stated that dilatation of the pharyngeal orifice
of the Eustachian tube was not feasible, and they sometimes denied the
efficacy of a curettage of the fossa of Rosenmuller. How could there
be such a thing as a palpable Eustachian orifice when it was all one could
to to understand the workings of the auditory apparatus?
Lymph Drainage of the Eyelids
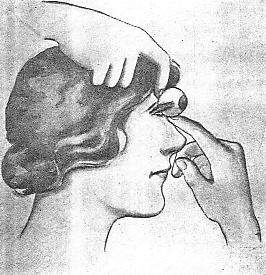
In blepharitis marginalis, chronic catarrhal conjunctivitis, trachoma, dacryocystitis, chalazion, hordeolum, and other infections it is essential that lymphatic drainage of the tarsus be re-established. Finger surgery of the upper lid, in addition to structural adjustments, has worked wonders in the treatment of external diseases of the eye. To treat the upper lid, the nail of the little finger
should be trimmed below the cushion, and the phalanges thoroughly cleansed
and lubricated with some mild antiseptic fluid. (Incidentally, I
may remark that I have found the Williams antiseptic fluid very efficacious
in this technic.) The first phalanx of the little finger (palm upward)
is gently passed beneath the upper lid, upward and backward, to the supraorbital
space. The thumb and forefinger of the opposite hand supports the
upper lid, feeding it over the little finger during the insertion.
The interference and purchase power of the inferior palpebra can be avoided
by depressing the lower lid with the index finger of the left hand, and
as this is done the little finger of the right hand will pass into space.
The thumb and forefinger of the opposite hand, resting upon the upper lid,
act as a fulcrum and guide, and, by raising the hand of the inserted finger
(the phalanges being held rigid), the traction is referred to the inner
and outer canthus, and the tarsus is treated by rolling the upper lid over
the inserted finger. (Plate 50).
An instillation of a fifty-per cent solution of alkalol
(not alcohol), a few drops in each eye, is used as a prophylactic measure
following each treatment. The alkalol is very soothing, and will
not discolor the conjunctiva like instillations of the silver salts (argyrol).
The Ocular Lymphatics Lymphatics have not been found in the cornea. In the conjunctiva, lymphatic vessels are present. Elsewhere in the ocular structures their places are taken by lymph spaces, which form two systems -- an anterior and a posterior. Ball says that the lymph from the anterior segment
of the globe collects in the anterior and posterior chambers, whence it
passes through the ligamentum pectinatum into the canal of Schlemm.
From this channel it passes into the anterior ciliary veins.
In the treatment of glaucoma, optic nerve atrophy,
choroiditis, cataracts, and other nonsuppurative processes, finger surgery
of the globe is the technic par excellence. Frequently, where only
failure results from other modes of therapy, excellent results are obtained
by this new osteopathic treatment of the ocular lymph spaces.
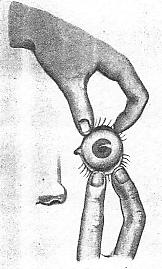
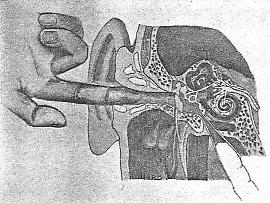
PLATE LIII. Finger surgery of the external auditory meatus. The forefinger is dilating the meatus in the treatment of the lymphatics of the auricle and canal. In the treatment of the ocular lymphatics the writer elevates and dislocates the eyeball, the forefingers of both hands retracting and depressing the upper and lower lids as the globe is gradually lifted out of its cavity and upon the rim of the orbital fossa. The eyeball is allowed to remain in this position until there is a marked injection of the conjunctiva, indicating a change in the vascular supply. The orbit is easily replaced by releasing the lids, applying careful and steady pressure on the sclera and a slow rocking movement to the globe. (Plates 51, 52). These manipulations will relax the musculature and deep tissues of the orbital cavity, re-establish the lymph spaces, filtration angle, and normal exits, correct the physiologic astigmatism, which is due to lid pressure, and adjust the axial ametropia, which is due to malalignment of the extrinsic muscles. A few drops of a two per cent solution of holocain or alypin, allowed to remain a few minutes, will very readily anesthetize the tissues, and the eyeball can be elevated and dislocated with very little dicomfort to the patient. I have administered this local manipulation of the eyeball three times a week for six months or more, and it is very gratifying to see the globe change from a passive to an active congestion and observe the elimination of the orbital discomfort, with marked improvement in vision and often with the complete removal of the glasses. The structural adjustments (osteopathic lesions) were, of course, the supportive measure in every case. PLATE LIV. Millards
bimanual technic. The forefinger of the right hand is dilating the
right external auditory canal, while the forefinger of the left hand is
dilating the pharyngeal orifice of the right Eustachian tube (same
side), in the treatment of catarrhal deafness. The lymphatics
at both ends are treated at the same time, and the peripheral inhibition
stimulates the center.
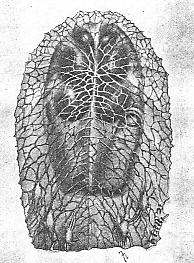
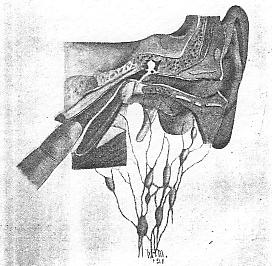
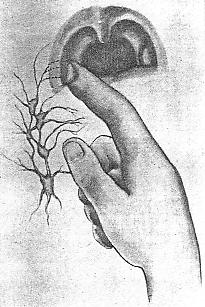
Lymphatics of the Auricle and External Auditory Canal The lymph drainage of the pinna and external auditory meatus is very closely associated with the lymphatics of the mastoid process and parotid gland. Inflammatory affections of the external meatus will, as a rule, invade the lymphatics of the neighboring tissues. Politzer says that the lymphatics of the anterior and superior walls of the meatus, the tragus, and the surrounding parts empty into the preauricular glands (on the parotid); that those of the lobule, the helix, and the inferior walls of the meatus empty into the infra-auricular glands (in the angle of the jaw); that those of the antihelix and the concha empty into the mastoid glands (on the apex of the mastoid process); and that those of the posterior wall of the meatus, together with those of the Eustachian tube, empty into the deep cervical and retropharyngeal glands. The tympanum is drained by the lymphatics, which pass out through the external auditory meatus to join the superficial glands of the neck. The lymph drainage of the labryinth is closely associated with the subdural and subarachnoid spaces of the brain. PLATE LV. Lymphatics
in the walls of the pharynx with the view looking forward to the
posterior nares from the cervical vertebrae position. The lymphatics
have been separated from the membranes. The forefinger is dilating
the right Eustachian orifice. This cobweb picture is very unique,
and is shown for the time in any text.
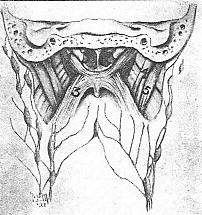
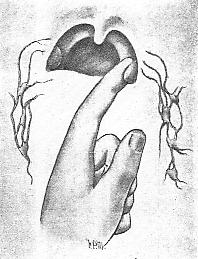
Finger Surgery of the Auditory Lymphatics In addition to structural adjustments (mandibular, clavicular, cervical, and upper-dorsal), digital dilatation of the external auditory meatus is an adjunct par excellence in the treatment of diseases of the external auditory canal, drumhead, and tympanum. Otitis externa circumscripta and diffusa, tinnitus aurium, myringitis, and catarrhal deafness have responded to this local manipulation. Before attempting a digital dilatation, the canal should be carefully examined for foreign bodies, be freed from wax, and dry swabbed. The index finger should be thoroughly cleansed, with nail trimmed below the cushion, and not lubricated. To enter the external auditory meatus, the operator stands at the head of the table, with the patient in a recumbent position. The index finger (palm upward) is slowly and carefully inserted, and directed upward and backward, with gradual rotation, from the operator toward patients shoulder. During the rotation, which is the knack of the technic, the operator should not use his wrist, but slowly lean forward as the finger passes upward and backward into the canal. The finger should not be instantly withdrawn, but allowed to remain a minute or two in location, and the technic should be repeated several times at each treatment. (Plate 53). To properly dilate the external auditory meatus requires, as a rule, from six to twelve treatments, but this technic should not, however, be administered more than three times a week. It will often be found difficult to enter the canal, but slow and careful insertion, with gradual rotation, will allow the tissues to accommodate themselves without surgical trauma. Immediately following the dilatation of the external auditory meatus, there will be a marked injection of the drumhead -- acute myringitis -- which is readily seen with the myringoscope. The active hyperemia thus produced flushes the tympanic membrane and ossicular chain, breaking up the low grade ossicular synovitis, tightening the over-relaxed drumhead, and releases the impingement of the lymph drainage of the external auditory canal and membrana tympani. The bimanual treatment as originated by Dr. F. P. Millard -- dilatation of the pharyngeal orifice of the Eustachian tube and external auditory meatus -- as reported in the Journal of the American Osteopathic Association (July, 1918), is now used by the writer, and is very efficacious in the management of catarrhal deafness. (Plate 54). PLATE LVI. Posterior nasal spaces and lymph drainage of muscles of palate and pharynx. (1) Levator veli palatini; (2) tensor veli palatini; (3) pharyngo palatinus; (4) stylo pharyngeus; (5) digastricus. PLATE LVII. Musculature
of the pharyngeal orifice of the Eustachian tube and lymph drainage
of the palate. (1) Superior constructor of the pharynx; (2) salpingopharyngeus;
(3) levator veli palatini; (4) pharyngopalatinus; (5) tubercle of Gerlach
(tube tonsil). During the act of deglutition, and as the soft
palate elevates, the tube tonsil comes forward and overrides the
Eustachian orifice, thereby preventing the regurgitation of foreign
substances into the Eustachian canal -- epiglottis of the tube.
The muscles which open and close this slit-like orifice are covered with mucous membrane, and form anteriorly the plica salpingopharyngeal and the plica salpingopalatine, which descend respectively from the lower end of the Eustachian cushion and from the anterior border of the Eustachian orifice to the soft palate and nasopharynx. (Plate 56). The lumen of the cartilaginous portion of the Eustachian
tube is entirely dependent on the proper relation of the muscles and tube
tonsil. Between the tube tonsil and posterior wall of the pharynx
is a recess -- fossa of Rosenmuller -- which is subject to great individual
variations in size, and is rich in glandular tissue. Chronic nasopharyngeal
catarrhs often give rise to the cystic hypertrophy of the adenoid tissue
and the formation of large gaps (pus pockets) and bridge-like bands in
the Rosenmuller fossa, which may interfere with the function of the tube
tonsil. Recent research has demonstrated conclusively that the Eustachian
cushion (tube tonsil of Gerlach) is the epiglottis of the Pharyngeal orifice
of the Eustachian tube. (Plate 57).
During the act of deglutition, and as the soft palate elevates, the tube
tonsil comes forward and overrides the Eustachian orifice, thereby preventing
the regurgitation of foreign substances into the Eustachian canal.
PLATE LIX. Cross technic.
The forefinger of the right hand is dilating the pharyngeal orifice
of the left Eustachian canal, with the patient in a recumbent position.
By turning this illustration upside down, the technic will be more
easily understood. This has many advantages over the lateral
technic -- left orifice with the left finger, etc.
Finger Surgery of the Eustachian Lymphatics
To dilate the right Eustachian orifice, the left forefinger is passed behind the uvula upward and backward into the nasopharynx. The wrist-joint and phalanges being held rigid, the weight of the operators arm will force the tip of the first phalanx into the pharyngeal orifice of the Eustachian tube. This cross technic will permit a much easier dilatation of the orifice without a tear in the plicas, which very often occurs in the lateral technic, and thus avoid the accumulation of granulation tissue within the cartilaginous portion of the Eustachian tube, which retards the results of the operative procedure. The fossa of Rosenmuller should, however, be cleaned with the alateral technic, and incidentally I may remark that Ballenger (1914 edition) in connection with this point uses the following language on page 684: Thomas H. Brunk first, and later W. S. Bryant, called attention to the presence of granulation tissue and adhesive bands in the Rosenmullers fossa, claiming that their removal with the finger introduced through the mouth relieved tubal catarrh and deafness. Indeed, this opinion is attracting considerable attention, as the removal of these bands has in numerous cases been followed by improvement. The adhesive bands are frequently present, and should be searched for more frequently than has been customary. On page 687 he says: If adhesive bands are present in the Rosenmullers fossa, the index finger of the right hand should be introduced through the mouth and the right fossa thoroughly curetted with the nail. The left index finger should be used to curette the left fossa. The operator, when manipulating the soft palate,
should avoid touching the posterior pharyngeal wall, which, when disturbed,
influences nausea and gagging, being the gagging center. The forefinger
should be passed to the lateral aspect of the uvula, then gently behind
the velum pendulum palati, and upward and backward into the nasopharynx.
While forcibly springing the soft palate, the traction should be exerted
upon the lateral muscular portion, and not the raphe of the velum.
Traction exerted upon the uvula or raphe of the velum will have little,
if any, effect upon the walls of the nasopharynx. The muscular portion
should be forcibly sprung downward and forward, forming an acute angle
with the hard palate, and held in this position a minute or two.
This will influence the lymph drainage and eliminate the passive congestion
within the lateral nasopharyngeal walls. (Plates 60,
61, 62).
PLATE LXI. The forefinger
is springing the soft palate, downward and forward, forming an acute
angle with the hard palate. The operator should avoid touching the
posterior pharyngeal wall -- the gagging center.
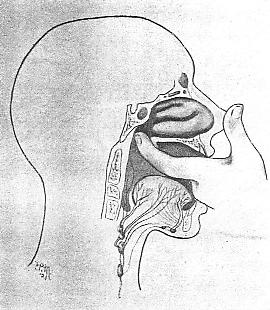
Most of the lymphatics of the nasal fossa enter the
retropharyngeal glands placed behind the pharynx, in front of the rectus
capitis anticus major, and hence retropharyngeal abscess may arise in consequence
of diseases of the nose. Other lymphatics go to the submaxillary,
parotid, and upper deep cervical lymph glands, and it is common to find
these enlarged in nose affections, especially in those of a scrofulous
nature. The lymphatics of the nose also communicate with those of
the meninges through the cribriform plate. (Treves).
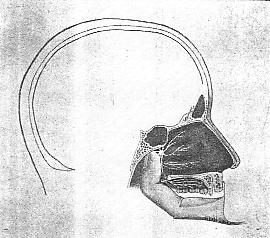
Finger Surgery of the Nasal Lymphatics Digital dilatation of the posterior nares by means
of the index finger, and anterior nares with the little finger, is very
efficacious in the reestablishment of the lymphatic drainage of the nasal
cavity. The writer uses this technic, in addition to structural adjustments,
in the treatment of catarrhal deafness, hay fever, otitis media, pharyngitis,
and other diseases of the upper respiratory tract.
PLATE LXII. Finger
surgery of the oral lymphatics. The forefinger of the right hand
is passed behind the uvula, upward and backward, into the nasopharynx,
and the soft palate is sprung, downward and forward, being held in
this position from one to two minutes.
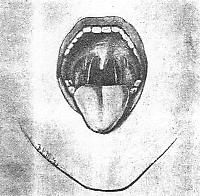
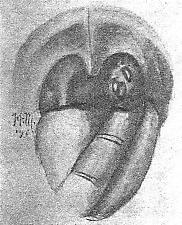
Lymph Drainage of the Oral Cavity The lymphatic channels of the oral cavity pass into the lymphatic glands situated at the angle of the jaw, and this accounts for the enlargement of the glands here in certain affectons of the nasopharynx. The lymphoid tissue is in scattered nodules, except on the lateral walls just behind the posterior pillars of the fauces, where a chain of lymph nodules runs vertically, connecting with the lymphoid tissue along the lateral walls of the nasopharynx. (Plate 64). The mass in the neck, often mistaken for an enlarged tonsil, is formed of enlarged glands, situated near the tip of the great cornu of the hyoid bone, and overlying the internal jugular vein. These glands receive the tonsillar lymphatics, and are almost invariabaly enlarged in all tonsil affections. The oral lymphatics pass chiefly to the upper cervical glands. Those from the upper part of the posterior wall join a few postpharyngeal glands, which are found on each side of the pharynx. The lymphatic glands of the neck drain the teeth, tonsils, adenoids, pharynx, and the mastoid region. PLATE LXIV. Lymphatics of the uvula, tonsils, and pillars of the fauces, and their relation to the lymph glands of the submaxillary and hyoid areas. The outlines in white are the structures treated by finger surgery in the management of uvula alteration, nasopharyngitis, hay fever, and catarrhal deafness. Springing the soft palate, downward and forward, will reestablish the lymph drainage of the nasopharynx and posterior nasal spaces. PLATE LXV. Diagram
of the submaxillary glands and their relation to the tonsillar lymphatics.
The forefinger is milking the tonsillar crypts.
Finger Surgery of the Oral Lymphatics The faucial tonsils are only a part of the lymphoid structures of the pharynx, and, owing to the continuity of this glandular chain, focal infections in neighboring lymphatic nodules are often the exciting factors in tonsillitis. (Plate 65). To demonstrate that the pharynx is a source of these infections, I shall briefly review the anatomical relations of the lymphoid tissues in this region -- the faucial tonsils, globular masses, situated between the anterior and posterior pillars of the fauces, on either side of the orophyarynx; the mass of lymphoid tissue on the posterior pharyngeal wall, commonly called adenoids; the lingual tonsils, situated at the base of the tongue, on either side of the the mass of the median line and the lymphatic nodules on the posterior and lateral walls of the pharynx. This group of tonsils makes up the so-called Waldeyers ring, and, to my mind, this is the Roman wall of the throat, which acts as a protective agent to the respiratory tract during early childhood. Bearing in mind the four cardinal factors in bacteriology -- namely, lowered resistance, avenue of entrance, virulence, and number -- it is readily seen that any break in this wall of lymphatic nodules exposes the system to almost everything on the infectious disease calendar. In considering this subject an effort is made not so much to direct attention to anything new in oropathology, but especially to consider the avoidance, as far as possible, of unnecessary surgery upon useful structures, and, most of all, to urge greater care in the matter of tonsillar diagnosis. (Plates 66, 67). Masland, reporting his tonsillar research, says: We see in the tonsil in the early years of life a startling picture of developmental change. In normal children, in connection with the lingual tonsils and the nasopharyngeal adenoids, this pharyngeal ring of lymphatics, Waldeyers is always of considerable size. Prominent in early years, it undergoes a retrogressive change, but there remains always some lymphatic structure throughout the ring. The thought has come to me of the possible iterrrelation, either or both interactivation and interinhibition, between this structure and the thymus and the thyroid, particularly in the early years of life. How far this has been investigated, I do not know. Can we deny, then, that this pharyngeal lymphatic ring, over which pass all ingested liquid, solid, or gaseous material, does perform a vital function in the body economy? PLATE LXVI. Finger
surgery of the tonsillar lymphatics in the treatment of chronic tonsillitis.
The forefinger is separating the plica trangularis and anterior pillar
of the fauces from the parenchyma, thereby releasing the impingement
of the subdivisions of the tonsillar artery and venous drainage.
TECHNIC. -- The author uses what is termed a suspension
technic, by which the tonsil is lifted from its infratonsillar fosssa
and held in this position for a minute or two. (Plate
69). This is easily done with no discomfort to the patient, by
passing the index finger into the mouth and following the side of the tongue
to the lower pole of the tonsil. The finger should not touch the
posterior pharyngeal wall -- the gagging center -- and the manipulation
should be restricted to the lower pole. With the cushion of the index
finger the tonsil is gradually raised and held in suspension for a minute
or two. In the bimanual manipulation counter pressure is made on
the outside of the throat, at the submaxillary area, with the index finger
of the opposite hand. The lingual tonsils and varix, situated at
the base of the tongue, may be treated with the same finger, not forgetting,
however, to avoid the gagging center on the posterior pharyngeal wall.
This technic will reestablish the lymh drainage, function of the plica
triangularis, and milking process of the tonsillar crypts.
The Lymph Drainage of the Larynx The lymphatics of the larynx are of much importance
with reference to voice alteration. The lymphatics above the cords empty
into two or three trunks in the aryepiglottic folds, which pass through
the thyrohyoid membrane to the glands on the internal jugular vein at the
level of the upper border of the thyroid cartilage. A small gland
is sometimes present on the thyrohyoid membrane, but appears seldom to
be infected. The lymphatics below the cords leave the air-tube above
and below the cricoid and empty into the lower deep cervical glands along
the jugular vein. Some pass with the inferior laryngeal vessels to a peritracheal
chain of glands; several minute glands may be found on the crithyroid membrane
and on the trachea, especially about the thyroid isthmus, but are rarely
involved. The vocal cords themselves lie between these two systems;
their lymphatics, which are remarkably small and scanty, pass to the upper
set of vessels.
PLATE LXIX. Finger surgery of the tonsillar lymphatics (suspension technic). The forefinger of the left hand is lifting the left tonsil from its infratonsillar fossa and holding it in suspension for a minute or two. This manipulation should be restricted to the lower pole, and the operator should avoid touching the posterior pharyngeal wall -- the gagging center. TECHNIC. -- The index and second fingers are passed over the posterior aspect of the tongue -- avoiding the gagging center -- and directly into the epilarynx. The hyoid is treated by a rotary movement of the fingers and epiglottis by a stretching of the epiglottidean ligaments. The middle ligament -- a prominent mesial fold of mucous membrane -- is often found to be indurated and resembling a tumefaction. A few treatments at this area will work wonders in voice failures and tickling throats. As the fingers are withdrawn, the structures of the epilarynx and those at the base of the tongue are treated by a forward forcible manual traction upon the posterior aspect of the tongue. The cushions of the index and second fingers are placed just beneath the varix and lingual tonsils, and with this purchase power the tongue is forcibly lifted upward and forward and held in this position for a minute or two, which will reestablish the lymph drainage of the larynx, varix, and lingual tonsils. The external aspect of the larynx is supported by the opposite hand, bringing counter pressure and raising the larynx as the tongue is brought forward, the opposite hand being, of course, on the ouside of the throat. This is one case where anesthesia, of any sort, is contra-indicated, as the peripheral stimulation excited by the digital insertion and manipulative procedure is an important factor in the treatment. If the tissues are anesthetized, they lose this stimulating effect, and the treatment will not be as efficacious. This local manipulation of the larynx has worked wonders in the treatment of acute and chronic laryngitis, many vocal celebrities and famous orators have been returned to their professions by this treatment. |
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}