
|
The anemias associated with certain abnormal conditions of the spleen and those due to parasites are not logically associated, except that in the latter group of anemias the spleen is often concerned in the pathology, and thus the final condition is partly parasitic and partly splenic in nature. This relation is particularly noticeable in malaria and in kala azar, though no cases of the latter disease have been studied in our laboratories. Several related diseases are included in this group. Originally the term was applied to all anemias in which the spleen was enlarged but with further study many of these abnormal conditions have been explained by a recognition of definite etiological factors. Several chronic infectious diseases cause enlargement of the spleen with some degree of anemia; tuberculosis, syphilis, malaria, kala-azar and hemolytic blastomycosis may be associated with splenic enlargement, anemia and no other prominent symptoms for long periods of time. In certain cases of cirrhosis of the liver, cardiac inefficiency and Hodgkins disease, enlargement of the spleen and anemia may e the most conspicuous symptoms for a time. Splenic enlargement is conspicuous in several of the leukemias and anemia usually occurs after the leukemia has been present for a time. The term splenic anemia should be limited to those
cases in which anemia and splenomegaly are associated with normal or low
white cell count, and with no other recognizable cause of either the anemia
or the splenomegaly.
The place of the spleen in the metabolism of blood cells has been studied by noting the effects of splenectomy in animals and by observing human beings with various abnormal conditions of the blood and of the spleen itself. Splenectomy in normal laboratory mammals is followed by marked decrease in the red cell count, usually to about two-thirds the number of normal to the animal. Leucocytosis to about three times the normal white count follows the operation within a few hours to a few days; this diminishes gradually within ten days or so to about twice the normal leucocyte count. The anemia and the leucocytosis gradually diminish and a normal count is usually present within two months in small animals, and within six months in large animals. Young animals show return to normal more quickly than do older animals. The reactions I man are complicated by the disease which was supposed to require splenectomy. The red blood cells become more resistant to hemolytic
agencies as a result of splenectomy. Urobilin in the urine is diminished,
indicating that the red blood cells are less rapidly destroyed.
There is diminished immunity to certain infections, in animals which have been splenectomized. This has not been definitely shown for human subjects but is probably true. Vertebral lesions affecting the circulation through the spleen and the liver are known to diminish immunity to the infectious diseases of childhood. Treatment of both normal and abnormal human beings which cause increased rapidity of the blood flow through the liver, spleen and pancreas increase the opsonic index and the leucocytic index for tubercle bacilli (Whiting). After splenectomy hyperplasia of other tissues of the reticulo-endothelial system occurs. The enlargement of the spleen which occurs during
the course of nearly all acute infectious diseases suggests its functional
value in reaction to infections. It should be remembered that this enlargement
may sometimes be due to infection, abscess and other pathological conditions
of the spleen itself, due to the disease or to some complication.
The place of the spleen in the control of the erythrocytic level of the blood is not yet well understood. Certainly the beneficial effects of splenectomy in splenic anemias with severe hemolysis suggests the possibility that an abnormal spleen may exert some abnormal inhibitory influence upon the erythrocytopoietic tissues. The increased resistance of the red blood cells to variations in osmotic tension and other test conditions after splenectomy is of interest in this connection. For this reason splenectomy was formerly employed as a therapeutic agent in pernicious anemia. Abnormal conditions characterized by splenomegaly
and anemia with no other etiological or other associated disease are rare,
and they are usually of developmental origin.
This disease has no known etiology. It is characterized by progressive anemia, enlargement of the spleen, hemorrhagic tendencies and cirrhosis of the liver with marked ascites Enlargement of the spleen first occurs and this may antedate the anemia by months or even by several years. Rarely the spleen may become greatly enlarged; usually it is not more than two or three times its normal size. Anemia is of the aplastic type with normal or low color index, few or no reticulated cells or normoblasts and neutrophilic leucopenia. The lymphocytes usually remain normal in actual numbers. Platelets show moderate reduction. The red cells do not show diminished resistance to hypotonic solutions. Eighteen cases of Bantis disease studied by Rowntree usually showed moderate degrees of oligocythemic hypervolemia. The findings varied from 67 cubic centimeters to 112 cubic centimeters of whole blood, and from 50 cubic centimeters to 83 cubic centimeters of plasma per kilogram of body weight. After splenectomy the blood volume diminished, with an average decrease of 7.4% in the whole blood and 17.5% of the plasma. Hemorrhages which are apparently spontaneous may occur from any of the mucous membranes. Hematemesis is especially common and this may lead to an incorrect diagnosis of gastric ulcer. Portal cirrhosis occurs rather late in the disease, sometimes twelve years or more after the splenic enlargement is first noticed, and is usually associated with ascites. Jaundice is slight or absent. Cachexia develops rapidly after the cirrhosis occurs and death may be due to this or to severe hemorrhage from stomach or intestines. At autopsy the spleen shows characteristic changes. The increase in size is partly due to the great amount of blood which it contains in its greatly dilated veins. The vasa brevia are enormously dilated. Great blood sinuses are found which connect the spleen with the stomach and the diaphragm. These increase the difficulty of splenectomy. Moderate hyperplasia of the bond marrow appears to be due to a reaction against the anemia. Fibrosis of the Malpighian bodies and of the trabeculae are the most important microscopic changes in the spleen. Splenectomy is the only adequate treatment and the
results of this operation are often satisfactory. The mortality is higher
than in many other operative cases, and the percentage of deaths increases
the longer the operation is postponed. After hepatic cirrhosis is recognizable
splenectomy is of little value.
In this disease there is a definite relationship between the enlarged spleen and the anemia, though the red blood cells are themselves of abnormal form and quality. Two types of the disease are generally recognized. Familial hemolytic jaundice (Chauffard-Minkowski type) follows Mendels law of heredity as a dominant type, though cases of the disease in which there seems to be no doubt of the diagnosis have been reported with no history of the disease in ancestors or in collateral relations. The acquired form (Hayem-Widal type) occurs during adolescence or later, and is somewhat milder in degree. No family history of the disease can be found. The disease is characterized by splenomegaly, hemotogenous jaundice, anemia and a greatly diminished resistance of the red blood cells to salt solutions. The splenomegaly may be slight or extreme, sometimes approaching the size of the enormous spleens sometimes found in leukemias. The jaundice exists in mild degree constantly but crises occur once to several times each year in which there is sharp increase in the size of the spleen with marked and sudden jaundice. The skin presents an orange or brownish tint rather than the green of ordinary obstructive jaundice. The serum, urine and stools contain greatly increased amounts of pigments. Sharp pains around the gall-bladder often suggest gall-stone colic. Gall-stones are frequently present in patients with hemolytic jaundice and symptoms due to the stones may cloud the diagnosis. The colicky pain may be very severe in cases with no gall-stones. Anemia is not typically of the secondary type. The color index remains at about unity. The red cells are peculiarly globular in form so that they appear smaller and of deeper tint than normal. While normal blood withstands hemolysis in salt solutions as low as (0.44%) or even less, these cells show hemolysis in salt solutions of 0.7% to 0.5%. The red cells are very fragile also on the warm slide. This peculiarity of the red blood cells is pathognomonic of the condition, and is not found in so marked a degree in any other disease. Reticulocytes and normoblasts are more common than in ordinary secondary anemia of the same degree. Megaloblasts, megalocytes, microcytes, poikilocytes are all rarely found in typical cases. The anemia is rarely severe The red cells may be diminished to three millions per cubic millimeter but may be almost or quite normal in number at times. The hemoglobin varies with the red cell count. During and for a few days after a crisis there may be a neutrophilic leucocytosis. At other times the leucocyte count is actually about normal but there is a moderate relative lymphemia. Platelets remain normal during the disease. The disease is rarely fatal and life seems hardly to be shortened by it. The crises occur one to several times a years, and they may last a few days to two or three weeks. During this time the patient is acutely ill with malaise, headache, fever, vomiting and sometimes sharp pains resembling gall-stone colic. The jaundice may be mild or very severe. There is no itching such as commonly accompanies obstructive jaundice. Recovery from the attack is slow. After the attack is over many patients seem to be in excellent health. Others are jaundiced, weak, anemic and subject to gall-bladder discomfort nearly all of the time. The accepted treatment is splenectomy in the familiar cases and in those acquired cases for which no pre-disposing other disease can be found. The results of this operation are usually excellent in the familial cases, and are occasionally good in the idiopathic acquired cases. The anemia, jaundice and crises usually cease at once and the patient rapidly becomes well and remains so. The red cells are always fragile and of spherical form, but they remain whole in the circulation and carry oxygen adequately. It is usually best to remove gall-stones at the same operation. The surgical work should be done during an intermission, not during a crisis. The treatment of those acquired cases in which some other disease seems to have a predisposing influence is that of the predisposing condition. Such diseases include malaria, tuberculosis, sepsis, dysentery, hookworm and other parasitic infections, syphilis, carcinoma and several others. Cholelithiasis has been considered predisposing, but it must be often true that the jaundice antedated the cholelithiasis. These diseases are so common while hemolytic jaundice is so rare that some predisposing factor, probably developmental, must be present in all, or nearly all, of the so-called acquired cases. The acquired cases are much more serious, as a rule, than the congenital. The crises are more acute and more frequent; the intermissions may not occur at all, and remissions be characterized by more or less severe symptoms. The anemia is more severe; sometimes the red cells reach less than one million red cells per cubic millimeter. The jaundice is less marked and resistance of the red cells to hypotonic salt solutions is more nearly normal than is the case in familial jaundice. The acquired form is not transmitted to the children. At autopsy, in both acquired and congenital cases,
the spleen shows hyperplasia and thickening of the capsule, and it is greatly
engorged with blood. The endothelial cells of the spleen contain great
numbers of red blood cells. The Kupffer cells of the liver show marked
siderosis. Both the erythroblastic and the leucoblastic areas of the red
bone marrow show abundant hyperplasia. The gall-bladder often contains
stones and its walls are thickened. The kidneys usually show some nephropathy
and their cells show siderosis in many cases.
This anemic leukemia of infants (anemia pseudoleukemica infantum) is probably not a distinct disease. There seems to be some developmental basis for the inability of these babies to react to infectious processes in a normal manner. This disease follows or is associated with some severe nutritional or infectious disease and is characterized by anemia of increasing severity, splenomegaly and myeloid leucocytosis, together with the symptoms of the underlying disease. It is possible that symptoms of severe malnutrition ordinarily supposed to be the cause of the anemia, may really be the earlier symptoms of the disease itself, as an entity due to developmental defect in the spleen and red bone marrow. That some developmental defect is an essential factor in etiology is suggested by the remarkably abundant myelocytes with relatively scanty leucocytosis, by the great diversity and the prevalence of rarity of Von Jackschs anemia among sick babies. The fact that several children in the same family may have this rare disease also suggests a developmental fault. The autopsy findings suggest a developmental basis for the peculiar blood and splenic changes. The red cells are greatly reduced, sometimes to less than half a million per cubic millimeter. Reticulocytes, normoblasts and various nuclear remnants within red cells are rather abundant; megaloblasts are rare. The blood picture may resemble that of pernicious anemia, which is, however, extremely rare in young children. The hemoglobin is considerably reduced and the color index is usually below 0.8. The leucocyte count may reach 50,000 or even 150,000 per cubic millimeter. Neutrophiles and neutrophilic and eosinophilic myelocytes predominate; hyaline cells include hyaline myelocytes and these may dominate the blood picture, thus suggesting lymphoid leukemia. The spleen is enlarged, sometimes slightly, more often very considerably. The liver shows some enlargement. The disease has a prolonged course. The predisposing disease passes into the anemic phase gradually. The splenic enlargement may be the first indication that anything more serious than delayed recovery from the underlying illness is present. Pallor becomes more marked, weakness and prostration increase, and the child often bleeds at the nose, or coughs or vomits blood, or blood may be found in the stools. Unless the nutritive condition improves the child may die of inanition within a few months. There is a tendency for improvement if conditions permit. No doubt with the development of the child the persistent embryological relations tend to diminish and disappear. About four-fifths of all cases recover within a y ear or two at most. Treatment is devoted to the underlying disease, plus an attempt to secure improved nutrition and better muscular tone. Lesions causing atony of the muscles of the splenic capsule have been reported in several cases under osteopathic treatment, and the course of the disease seems to be shortened by the correction of these lesions. At autopsy the spleen is found enlarged and great
areas of erythrocytopoietic and leucocytopoietic areas are found. The red
bone marrow is hyperplastic and may intrude upon the yellow bone marrow
quite extensively. The liver and the lymph nodes may also contain large
areas of hematopoietic tissue.
This is a disease of childhood, probably due to some developmental error, characterized by enormous splenomegaly, peculiar graying or bronzing of the skin, hemorrhagic tendencies and moderate anemia. The disease occasionally occurs in several members of the same family but it is not directly inherited, for obvious reasons. The enlargement of the spleen is greater than in any other disease. The enlargement of the liver seems to be secondary to the splenomegaly. The anemia is not severe until late in the disease. The bronzing of the skin often suggests Addisons disease. There is often pain in the bones and this may be extremely severe and persistent; it may be due to hemorrhages but is probably due to the pressure exerted by the tumor-like masses of cells within the marrow. Hemorrhages are rarely severe. Bruising of the skin occurs upon slight provocation; hematemesis and epistaxis occasionally may be quite severe. The disease has a slow progress but is inevitably fatal. At autopsy the spleen is found to be firmer than normal, with grayish, yellowish, whitish and brownish mottling. The whitish areas are composed of great masses of endothelial cells, twenty to forty microns in diameter, often arranged in alveoli but sometimes showing no definite arrangement at all. The protoplasm of these cells is crowded with vacuoles filled with some lipoid-like substance, probably a cerebroside. This trait gives them their name foam cells. The Malpighian bodies of the spleen show atrophy apparently due to the pressure of these cells. The brownish and yellowish areas of the spleen show hemorrhages in various stages of absorption. Cysts due to the degeneration of hemorrhagic areas are common. The liver, bone marrow and occasionally the lymph nodes show masses of these cells. They are occasionally found in the peripheral blood. At autopsy the developmental basis of the disease is strongly suggested by the finding of other developmental anomalies. Horseshoe kidney, cystic ovaries, uterine malpositions, cystic kidneys and various other developmental abnormalities are very common autopsy findings in these cases. The nature of the disease precludes any successful
therapy. Splenectomy seems to give some relief and to prolong life in some
cases. In other cases splenectomy has been followed by rapid increase in
the size of the liver and speedy death.
This resembles Gauchers disease somewhat. The two may be simply different types of the same disease. In Niemanns disease the foam cells are filled with a substance which gives the reactions for fats and the blood serum is definitely turbid from the pr essence of fat-like globules. The viscera, thymus, lymph nodes, bone marrow and sometimes the connective tissues show a peculiarly brilliant yellow color. These is no satisfactory treatment and death is inevitable from the nature of the conditions present. The child rarely lives to be more than two years old, or more than three months after the first symptoms are noted. Anemia due to parasites varies according to the location and the nature of the agents. Cats and dogs with abundant fleas suffer a severe anemia which cannot be differentiated from the anemia due to starvation, except that the eosinophiles are considerably increased. Human beings afflicted with lice and other parasites upon the skin also show secondary anemia of the starvation type, plus moderate eosinophilia. Parasites within the intestinal tract are generally
associated with blood showing the typical picture of starvation anemia,
plus eosinophilia which may be slight or extremely marked. The hookworm
and certain other intestinal parasites cause slight but chronic intestinal
hemorrhages; in such cases the anemia is of the hemorrhagic type. Several
flagellate unicellular organisms may infest the intestinal tract and these
frequently cause an anemia which is definitely of the pernicious type.
Bothriocephalus latus is a tapeworm, fortunately rare in this country,
which causes a condition resembling pernicious anemia in almost every respect.
Parasites of the blood itself include several very
different forms, and these diseases of the blood require especial attention.
This form of anemia was first described for patients in the clinic of The Pacific College of Osteopathy. The organism was found later in patients studied in the laboratories of The A. T. Still Research Institute in Chicago and in Los Angeles. Infection by blastomycetes has been reported many times in medical literature. In every case so reported the disease was fatal. The organisms vary somewhat, and all those previously reported have been almost or quite as large as ordinary yeast and have been pyogenic. The blastomycotic forms which produce this chronic anemia are not pyogenic and are not directly fatal. This organism (Blastomyces hemolytica) is very much smaller than ordinary yeasts. Both large forms and small forms of yeasts have been found in several malignant neoplasms and have been reported as having etiological value by several authors. They may, possibly, be concerned in producing the irritative influences which have some etiological value in certain forms of sarcoma and carcinoma but there is no reason, at this time, for supposing them important in the etiology of any kind of neoplasm. Blastomyces hemolytica can be isolated from the blood of persons infected and from scrapings from the tumor-like masses and the dry sores which are characteristic of the disease. Cultures made from these materials are of very slow growth and require from ten to forty days to become visible. They are facultative anerobes. The best culture media include boullion agar mixed with defibrinated blood; various gelatine preparations mixed with blood or with ascitic fluid, and defibrinated human blood alone. Culture media with pH of about 6.5 give better growth than those with pH of 7 or higher. Cultures are easily made of the organism in defibrinated blood alone; in these cultures the organisms attack the erythrocytes. Both the organism and the injured erythrocytes are phagocytized by the large hyaline cells and the neutrophiles in much the same manner as occurs in the circulating blood of the infected person. (Plate IX) Guinea pigs inoculated with the blastomyces hemolytica
show the symptoms characteristic of the infection in man and cultures from
their blood show the same characteristics as is the case with cultures
made from human material. These cultures produce the same symptoms in other
guinea pigs inoculated with them.
PLATE IX
Blood cells scraped from a tumor beneath the skin
of a human subject. N, a normal erythrocyte. Just above and to the right
is an erythrocyte showing the normal bowl-like outline of living red cells.
Several of the yeast-like organisms lie upon this cell. Other red cells
show different stages of destruction by the parasite, and the peculiar,
scalloped, semilunar remnants of the invaded erythrocytes.
The most pathognomonic symptom is the dry sore upon the skin. One or many such sores may be found. Occasionally the sores disappear in which case it may be difficult to secure a history of the initial skin lesion. The sore is characteristic. Usually a small lump is first noted just below the skin. This increases in size and the skin becomes eroded over the tumor. A dry scab forms, this drops off, only to be followed by another scab. These may be successively larger until an area of an inch or so in diameter may be concerned in the lesion. Rarely the sore exceeds an inch before the scabs begin to become successively smaller and finally the skin is healed over the area leaving no discoloration; if no pyogenic infection occurs there is no scar. Scrapings made from the tissues beneath the scab or from the tumor before the skin has become eroded show the characteristic yeast-like organism. Usually there is a secondary infection with staphylococci or other organisms after erosion occurs. The tumor-like mass beneath the skin contains only the blastomycotic organisms. The anemia is of the secondary type generally, except that on examination of many smears the organisms can be found within the red blood cells, the large hyaline and, occasionally, the neutrophilic cells. It is not easily recognized free in the plasma because of its small size and because it is often associated with the platelets in rather large groups. Fragments of red cells of characteristic forms may be found, and these should suggest the disease. The rim of the erythrocyte with its inner edge eroded in such a manner as to leave a scalloped outline is a very common findings in these cases. Cultures of blood showing these peculiar fragments may contain the parasite even though it may not be recognizable in blood smears. Inoculation of these cultures into guinea pigs produce typical symptoms of blastomycosis, and the autopsy findings are characteristic. The pigs must be killed; they rarely die as a result of inoculation of the blastomycetes alone. The lumps cause discomfort and dull or acute aching which varies according to the nerves of the area affected. They may appear anywhere, with no regard to the exposure of the skin to light or to irritation by clothing, or to the thickness of the skin; there is no difference between flexor and extensor surfaces or between the skin of the stunk and of the extremities. The lungs are occasionally infected, in which case the symptoms resemble those of pulmonary tuberculosis. Rales are usually more marked than in tuberculosis. The temperature curve is erratic and shows greater variations than is the case in tuberculosis. Night sweats are usually very severe. The euphoria characteristic of tuberculosis of the lungs is replaced, in blastomycosis, with a gloomy tendency which may approach actual melancholia. The organism can be cultured form the sputum. Inoculated guinea pigs show typical pathology. Weakness, pallor, muscular atony, anorexia, nervous
and emotional instability and motor restlessness suggesting hyperthyroidism
are common symptoms. Basal metabolism is not affected, however.
The infection has not, so far as has been reported, been the direct cause of death. The anemia and the pulmonary infection lower the resistance to other etiological factors and thus are predisposing factors. The manner in which the infectious agent gains entrance into the body is not known. In some study of yeasts used as foods in 1914-1915 in Chicago, similar organisms were found in beer and in commercial yeasts used for baking. Animals inoculated with these organisms did not show any symptoms of the dry sores nor of anemia, and cultures made from their blood did not grow. The tests were not completed and further work remains to be done before the organism can be described in detail and its origin definitely determined. Since the organism grows best on faintly acid media, increase of the alkalinity of the blood and the tissue juices of the patient is indicated. This is best done by means of diets including foods with alkaline ash and by avoiding an excess of those with acid ash. The circulation through the red bone marrow must be kept normal because the development of red cells to take the place of those destroyed by the blastomycetes must be encouraged. The food must provide a normal amount of iron and other minerals in the form of hemoglobin, myohematin and chlorophyll-containing vegetables for the same reason. Since the lack of oxidation results in the formation of sub-alkaline or acid katabolites t he patient must have good air and must breathe properly. No method of destroying the organism directly without injury to the patient has been found. The scabs may be scrubbed off from the sores and
the bleeding area washed with alkaline lotions. Weak carbolic acid lotions
are often nothing and may exert some antiseptic influence. Any comfortable
applications may be used.
Mrs. H. History of peculiar dry sores following small lumps which appear beneath the skin. Occasionally blisters occur instead of dry sores. These become purulent within a few days. This patient lived in a distant city. Hemoglobin reported as being 68%; no other blood examinations made. Smears were taken from the pus,s blood and serum from a non-purulent blister and were sent, under aseptic conditions, to the laboratory of the Institute. Cultures were made and a growth of Blastomyces hemolytica occurred. The cultures were used for several experiments. Cultures from pus were added to normal human blood which had been defibrinated by beating and the mixture incubated for thirty minutes at 38 degrees C. Smears were then made and examined. The erythrocytes showed invasion by the blastomyces. The large hyaline cells had phagocytosed both the parasite and fragments of erythrocytes. A few neutrophiles also phagocytosed a few of the parasites and had ingested the erythrocyte fragments abundantly. Cultures from the blood of Mrs. H. were added to normal human blood which had been defibrinated, and the mixture was incubated for 24 hours at 38 degrees C. The erythrocytes were abundantly invaded and the large hyaline cells had ingested many of the organisms; the neutrophiles had ingested the fragments of red cells abundantly, and also a few of the parasites. These tests were repeated for different temperatures and for different periods of incubation. Normal human blood in normal salt solution was mixed with a culture of the blastomyces and a hanging drop preparation was watched for several hours. The yeast cell adhered to the erythrocyte and as it grew the substance of the red cell disappeared very slowly in the immediate vicinity. The yeast cell then grew into the red cell and began to divide. Defibrinated blood from a normal guinea pig did not provide a good culture medium. The cultures from the blood of Mrs. H. were mixed with defibrinated guinea pig blood in various proportions and the mixtures incubated at several temperatures. The yeast attacked the red blood cells of the guinea pig but the leucocytes did not ingest the organism. The yeasts did not multiply in guinea pig blood during three weeks incubation. Inoculation of the ear of a guinea pig left a small
mass which slowly diminished in size and finally disappeared, leaving the
pig apparently uninjured by the infection. The pig was kept under observation
for four weeks and no symptoms appeared. Observation was then neglected
although the pig was still kept isolated. Ten days later the pig died.
At autopsy a dry sore was found at the site of the inoculation. The body
was emaciated and the lungs were congested. No hepatization was present.
Smears from the sore on the ear, from the lungs and from the blood showed
the blastomyces present in each case. Pneumococci were also found abundantly
in the smears from the lungs, so the blastomyces was almost certainly not
the direct cause of death. No other guinea pig in the place had pneumonia.
Large hyaline cells . . . .. . .. . . . . . . . .
. . . . . 1.9% 158 per cu.mm.
Some organisms, nature not certain, present within the red cells and within a few of the large hyaline cells. Cultures were made of the blood and these were used for further tests. (Plate IX) On physical examination considerable edema was found; the skin was definitely purplish in tint, and a cardiac murmur indicated a mitral lesion. Sphygmogram verified this diagnosis. No history of syphilitic infection was secured. Patient is a widow with four children, all normal, no history of miscarriages or of still-births. Patient is janitress and works ten hours each night in an office building. Cultures made from blood of Mrs. B. were added to normal blood which had been defibrinated, and the findings already described in the case of Mrs. H. were repeated. Guinea pig inoculated in right ear. Four weeks later a dry sore appeared at site of inoculation. Pig became thin and anemic; was killed by ether anesthesia five weeks after inoculation. Smears from the lungs, liver, blood and spleen showed the characteristic organism. Smears from the spinal fluid, peritoneal fluid, pericardial fluid and from the brain did not show any of the parasites. Four puppies inoculated in the right ear with the
cultures from the blood of Mrs. B. Three showed no symptoms whatever though
they were kept under observation for three months. The fourth puppy developed
the typical dry sore at the site of the inoculation, became thin and pale,
and was killed by ether two months after the inoculation. The intestines
were full of small round worms and this no doubt was partly the cause of
the emaciation and anemia. Blastomyces hemolytica was abundant in the smears
from the lung and the blood. Cultures made from these cultures developed
the usual symptoms in guinea pigs.
Hemoglobin . . . . 72%
Cultures were made from one of the small lumps which
he reported as antedating each small scab-like sore. The characteristic
blastomyces invading red cells appeared in the smears and the culture growth
was characteristic. Inoculations into guinea pigs produced the typical
symptoms but not the death of the pig, which was finally killed at the
end of the fifth month, with ether. Smears from the lungs, blood and spleen
showed blastomyces. Cultures from these tissues produced similar symptoms
in other pigs. Smears and cultures from the brain, peritoneal fluid, kidneys,
cerebro-spinal fluid and gall-bladder were all negative.
Histoplasma capsulatum is a parasite somewhat resembling a certain stage in the development of the Leishman-Donovan bodies of kala azar, and producing a disease called histoplasmosis. This parasite was first described in the Isthmus of Panama by Samuel Darling in 1906. Since that time several cases have been described in the southern part of Mexico and Yucatan; one case was described in Wisconsin, in a patient who never had been in any other state or country. We had one case studied in the laboratory of The A. T. Still Research Institute in which the diagnosis seemed definite and one case in which the diagnosis was probable but in which no careful study was possible. Both these patients probably contracted the disease in Mexico. The symptoms include those due to cirrhosis of the liver, splenomegaly, invasion of the endothelial cells of the intima of the blood vessels and of the epithelial cells of the intestines and the lungs. Fever is occasional and may be very severe. Thrombosis produces nervous symptoms. Invasion of the endocardium is common. The parasite does not attack the red blood cells directly. It is engulfed by the hyaline cells of the blood but is not ingested by the neutrophiles. It is occasionally found free in the blood plasma. In one of our cases the symptoms included feverish
attacks, hepatic symptoms resembling those of cirrhosis, painless splenomegaly
of moderate degree, and a peculiar paralysis, which seemed to be due to
thrombosis. The parasite was found in the large hyaline cells of the blood,
but no further study could be made of the case. The man is still alive
after three years. In another case some further study was made, but no
autopsy was permitted.
H 13 age twelve years. At first examination was apparently very ill, with constant fever varying between 99 degrees F, and 102 degrees F. Spleen and liver much enlarged and painful on pressure. The spinal tissues between the fifth thoracic and the third lumber segments were tense and hypersensitive. Cardiac sound indicated valvular lesions involving the mitral valve and at least one other valve, probably the tricuspid. Pulse varied between 102 and 120, respirations irregular, from 78 to 32 per minute. History of her childhood was uneventful, except as follows. Her parents took her to Mexico when she was three years old, and she lived there for eighteen months. She was then taken to Chicago. She was never robust but did not seem definitely ill. At the age of seven years she had measles and this was followed by attack which was thought to be acute articular rheumatism of typical form. This left her with a valvular heart lesion. (Instead of having acute articular rheumatism of atypical form she may have suffered from histoplasmosis at that time.) No careful study was made of the condition. During the next three years she improved in general health and the cardiac symptoms diminished in severity. This last attack began a few weeks before she was first examined. There was first increased severity of the cardiac symptoms followed by increasing fever, increasing size of the abdomen and severe headaches. Blood and urine examinations were made soon after the first physical examination, with results as follows: Blood examination.
A parasite which most nearly resembles the Histoplasma capsulatum of Darling is present within the splenocytes and the large hyaline cells of the blood. (Plate X) Uranalysis
A few parasitic organisms like those found in the
blood are present within the renal epithelium and within certain large
hyaline cells apparently derived form the blood.
Late in the afternoon of May 4, three drops of urinary sediment were injected into the peritoneal cavity of two guinea pigs and two drops were injected into the ear veins of the same animals. No ill effects followed until the morning of May 9, when it was noted that the pigs were inactive. Both were feverish with rapid pulse and respiration. Both died during the afternoon of that day and were examined at once. The findings were identical for both. All viscera were intensely congested and hemorrhagic areas were abundant. Smears were made of the blood, urine, and saliva. Smear preparations were made from the lungs, pericardial sac, endocardium, peritoneum, spleen, pancreas, liver, kidneys, adrenals and thymus. Smears from the saliva and the pancreas did not show
the organisms. All other smears showed endothelial or other hyaline cells
containing from one to five parasites like those found in the blood of
the patient. The smears from the blood and the urine also showed these
organisms. (It may be stated in this connection that our guinea pigs do
not show the Kurloff bodies in their blood, and that the organism in question
does not resemble the Kurloff bodies.) (Plate XI)
On May 29, blood from the patient was inoculated into the right ear vein of a guinea pig. No effects were noted until May 22 when the pig was inactive and feverish with rapid pulse and hasty labored respiration. Blood smears were prepared from the skin of the left ear. Parasites were found in 1.4% of all the hyaline cells. No parasites were found within the granular cells. The pig did not die but remained feverish and ill. On June 10 chloroform was given and the pig quickly succumbed. Viscera were less severely congested and less abundantly hemorrhagic than in the pigs inoculated with urinary sediment. Spleen considerably enlarged, to approximately three times the normal size. Tricuspid and aortic valves showed evidences of acute inflammation. Smears were made from viscera as in the pigs with urinary inoculation, with same findings, except that the parasites were about three times as abundant. Both the urinary sediment and blood from the patient, and urine, blood, scrapings from various viscera and the cerebro-spinal fluid from all three of the guinea pigs were inoculated upon and into various culture media but none showed any sign of growth. These same materials were inoculated into ten other guinea pigs, but none of them succumbed to the disease and the parasite was not found in the cells of these pigs at any time. They were killed and the tissues examined at intervals of one week for two months. This parasite differs from that described by Darling in form. Darlings descriptions and the photographs made of cells containing the parasite show it to be oval or roundish, while this parasite, in the hyaline blood cells and the epithelial cells of the urine, was somewhat angular, with fine processes extending from the central body almost or quite to the wall of the capsule. The parasite are so much alike, however, that they should be tentatively considered identical. A diagnosis of histoplasmosis was made and the prognosis
was gloomy. Treatment was chiefly symptomatic and devoted to the relief
of the pain with rest for the heart. Cardiac symptoms were followed by
left hemiplegia with symptoms suggesting embolism and death occurred about
thirty days after the first examination. No autopsy was permitted. No other
member of the family showed any evidence of the disease.
Malaria or paludism has been known for many centuries. Both names suggest the older idea that malaria is due to the emanations from marshy land. These emanations were supposed to be most dangerous at night and the dangers of night air were seriously discussed. The discovery of the plasmodium malariae by Laveran in 1880 paved the way for adequate study of the parasites which cause different forms of malaria and the final control of the disease through sanitation. The complicated life history of these parasites, the manner in which they are transmitted from human host to mosquito, and from mosquito to human host and the remarkable rigors and fevers which are caused in the human host by the physiological events of the life of the parasite while it is in human blood make up one of the most fascinating chapters in biology. Cases studied in the laboratories of The A. T. Still Research Institute, in Chicago and in Los Angeles, include chiefly old, atypical malaria. Recent acute attacks are not found often because there are no anopheles mosquitoes in the vicinity of these cities. Many cases of old and atypical malaria are found
and these present typical changes in the blood. The patients suffer from
vague symptoms of malaise and headache, dull aching in the region of the
spleen and the liver, and irregular attacks of chilliness of feverishness
or both. These symptoms are often so vague and so atypical that malaria
is not suspected until the blood examination shows the presence of the
characteristic organisms or of the call relations usually associated with
chronic malarial infection. Very often several examinations of blood taken
at different times are necessary before the organisms can be found. The
characteristic cell relations are present always.
Plasmodium malariae, the smallest of the malarial parasite and the one which is less commonly found, is most easily recognized by the rosette-like arrangements of the schizonts within the erythrocytes. Plasmodium vivax is not easily differentiated from plasmodium falciparum in smears taken from these old, atypical cases. The history of the early disease usually indicates which of these organisms is present. Plasmodium malariae causes the quartan type of fever, the plasmodium vivax the tertian and the plasmodium falciparum the aestivo-autumnal or malignant type of malarial fever. Quotidian fevers are due to double infection b the vivax or triple infection by the malariae. The intervals between the attacks are measured by
the time required for the completion of the asexual cycle. In old cases
the period required for the asexual cycle seems to vary for different organisms
in the blood at the same time, so that instead of the definite chill followed
by the definite fever there are irregular attacks of chilliness or feverishness
or both, with varying symptoms of malaise, headache and perhaps some dull
pain or aching in the region of the spleen.
In these late cases the blood changes may be quite significant. The large hyaline cells and the intermediate sizes of hyaline cells called splenocytes are considerably increased, both actually and relatively. These cells often contain fragments of red blood cells or granules of pigment derived from the hemoglobin of cells previously ingested and destroyed. The blood serum may be stained brownish and this is due to methemoglobin or some related compound. The granular cells are often diminished both relatively and absolutely. They rarely contain erythrocyte fragments. They are often irregular in outline and have swollen nuclei with frayed edges. The neutrophile granules are often rather irregular in size, especially in those cases which are characterized by a rather large spleen. Fragments of red blood cells may be found, and these may suggest the diagnosis. The malarial parasite is occasionally found, and the diagnosis is then definite. In many instances patients suffering from vague and indefinite symptoms show blood with these traits, and the search for the malarial organisms should then be very thoroughly carried on. It may be necessary to study blood specimens taken at different times of the day and on different days in order to secure a specimen in which the parasites can be found. If any chilliness or feverishness occurs, the blood should be taken just before such attacks are expected, or at as nearly this hour as is practicable. Vigorous osteopathic treatment, of a kind planned to cause rapid blood flow through the spleen, often causes the parasite to appear in the peripheral blood. Such treatment exercises a definite therapeutic effect upon the patient, no doubt partly because the parasites are thus driven into the peripheral blood, and through many tissues where they are subjected to the various parasiticidal agencies of the body. The length of time during which the malarial organisms
can remain in human blood is not known. In our clinics patients have been
found with malarial organisms in the blood who had shown no recognizable
malarial symptoms for twenty and even for fifty years. Many of these patients
had not lived in a malarial country for many years, and have not known
that they had been exposed to the possibility of infection during that
time. It is, however, easily possible that re-8nfection occurred during
some journey to malarial districts. Re-infection cannot be certainly excluded.
It is significant that nearly all of the patients in whom old, atypical
malarial parasites have been found are those who have suffered very severe
malarial attacks in early life.
Recovery from malarial invasion depends upon several factors which differ somewhat from those which protect the body against bacterial invasion. It should be remembered that in bacterial diseases the neutrophiles ingest the bacteria, that various agglutinins, opsonins and precipitins are developed within the body, and that these seem to be of considerable value in immunity. In malarial invasion and in other forms of animal parasites the body cells do not react in the same manner. The neutrophiles are phagocytic only very inadequately, if at all, for animal parasites. The large hyaline cells, the epithelial cells and the splenocytes are the chief phagocytes for malaria and other animal-like parasites of the blood. The only physiological reaction of the body as a whole is the development of the fever. The high temperature often present during a malarial fever is fatal or at least very harmful to the parasites, and this is one important factor in preserving human life in malarial countries. It is, of course, frequently an inadequate reaction, and the fever itself may destroy the more delicate cells of the body. But it does help to destroy the parasite and it does facilitate the oxidation of the wastes of katabolism. The liver and the spleen are the most efficient of
the protective agencies within the body against malaria. These organs remove
the fragments of the injured red cells from the blood and transform the
various substances derived from them into harmless materials to be excreted,
or into substances fit to be utilized again in the manufacture of new cells.
The spleen provides a constant supply of active hyaline cells which are
able to ingest and destroy the malarial parasites. The increased activity
of these organs during a malarial attack is evident. The enlargement of
both is a very common symptom. This increase in size is in part due to
the increased activity caused by the blood destruction, and is in part
a reaction to the invading organisms and the products of their activity.
In order that the liver and the spleen may react efficiently it is necessary that they have a normal circulation of good blood through their tissues. The most serious cause of circulatory disturbance of the spleen and the liver is the presence of osteopathic lesions of the seventh to the ninth thoracic vertebrae and the related ribs. Patients who have such lesions are unable to react efficiently to malarial attacks, because these lesions disturb the circulation through the liver and the spleen. They also disturb the normal control of the non-striated muscle fibers of the splenic capsule, the gall bladder and the ducts of the liver. The red bone marrow must renew the supply of the blood cells in order that anemia may not follow the destruction of so many erythrocytes by the parasites. This means that the circulation and the innervation of the red bone marrow must be kept as nearly normal as is possible. Suitable food is also necessary; any ordinarily varied, wholesome diet, rich in proteins, provides the materials necessary for the renewal of the red blood cells and the hemoglobin. The adequate treatment of malarial patients must
include the correction of those lesions which interfere with normal circulation
of the blood through the liver and the spleen, and with the circulation
and innervation of the cells of the red bone marrow. This treatment prevents
excessively high temperatures in all but the most overwhelming malarial
invasions. Moderate degrees of pyrexia are undoubtedly helpful in destroying
the parasites, both directly and by facilitating phagocytosis by the hyaline
cells of the blood and the tissues.
Mrs. A., a woman fifty-four years of age, suffered a rather mild attack of influenza. She did not recover properly and for some months complained of irregular attacks of feverishness and chilliness, with varying headaches, malaise and discomfort in the region of the spleen. At the age of seven years she had suffered for several months from malaria. At that time the spleen was considerably enlarged, so that her dresses had to be made over and she felt humiliated by the large size of the abdomen. She had received enormous doses of quinine at that time, until the ears were seriously affected. The quinine was not given after the ear symptoms became serious, and the malarial attacks did not cease until cold weather came, which was nearly two months after the cessation of the quinine. PLATE X
During the seventh to the tenth years of her life she had malaria every summer and well into the autumn. After her fourteenth year she had excellent health wit only occasional accidental illness,--one or two attacks of food-poisoning, injuries from falls and strains, and one broken arm. On physical examination some weeks after acute influenza at the age of fifty-four years, the spleen and the liver were both found somewhat enlarged, hypersensitive to pressure, and firmer than normal. The skin was sallow and the conjunctivae yellowish. There was an area of marked spinal rigidity extending from the sixth to the twelfth thoracic segments. Blood examination made the day after a feverish attack showed no malarial parasites. Other smears were made at different times, until a smear was secured just as an attack of chilliness was beginning. These smears contained many parasites recognizable as plasmodium vivax. The white cell count was 4,500 per cubic millimeter. The differential count gave the following figures, based on a count of 500 cells: Large hyaline cells . . . . . . . . . . . . . . .
. . . . . 18 %
In counting 500 white cells there were found 20 red cells containing the plasmodium. The hygienic conditions and the diet of the patient were satisfactory and no change was directed. Treatment was devoted to the anatomical conditions. The spinal rigidity was treated by the usual osteopathic manipulations. The circulation through the liver and the spleen was brought to normal by suitable manipulations which provided more adequate venous and lymphatic drainage. The spinal rigidity and the symptoms diminished after the first treatment. The liver and the spleen returned to normal size during the first week. After the third day no chills or feverishness appeared. During the next six years the blood of this patient
was examined at irregular intervals, twenty times in all. Usually no parasites
were found in the blood. After a time of pronounced over-work with marked
fatigue, after an attack of measles, and during a period of marked depression
following a death in her family the organisms reappeared in the peripheral
blood, and vague, indefinite symptoms of chilliness, feverishness and headache
were noted.
Trypanosomes are flagellate unicellular organisms which usually live alternately upon vertebrate and invertebrate hosts. Many of these are pathogenic for man and for animals. Pathogenic trypanosomes are not endemic in this country but they may be brought from the tropics by infected persons. In such cases the symptoms may be very perplexing and diagnosis difficult. The sleeping sickness of Africa is caused by one of two trypanosomes, Trypanosoma gambiense, which is carried by the tsetse fly, or Glossina palpalis, and T. rhodiense, carried by G. morsitans. Another trypanosome which is transmitted by G. Tachinoides has been called T. nigerense, but there is good reason to believe that this is really identical with T. gambiense. T. gambiense has been divided into two groups, Castellanella gambiensis, which causes a more chronic and less severe form of sleeping sickness, and C. castellanii, which causes a more acute form of the disease in the human race, and which is speedily fatal to laboratory animals. Another trypanosome, T. bruccei, causes the terribly severe disease of horses and cattle in Africa. It is carried by G. morsitans and is supposed by many authors to be identical with T. rhodiense found in human blood. These trypanosomes all affect the blood of the mammalian
host. All have a peculiar body called variously kinetonucleus, parabasal
body, micronucleus or blepharoplast. This structure takes nuclear stains,
is smaller than the true nucleus and lies near the blunt end of the organism.
There is a tiny granule near the parabasal body and from this granule there
arises an undulating membrane. The flagellum borders the undulating membrane
and extends for some distance beyond this membrane at the end opposite
the parabasal body. The flagellum and the undulating membrane may be absent
during certain periods of the life of certain trypanosomes. The organisms
vary from fourteen to forty microns in length, and are two or three microns
in diameter. The nucleus is round, roundish or oval, and, in the oval forms,
the long diameter of the nucleus forms a right angle with the long diameter
of the body of the parasite. All of these structures are best studied in
the organisms secured after experimental inoculation of rats. In laboratory
animals T. rhodiense usually causes an acute disease, speedily fatal, while
T. gambiense inoculations are often unsuccessful and, in successful cases,
cause a chronic disease of slow progress.
The tsetse fly which feeds upon infected mammals may transfer the infection immediately to another mammal. After a few hours this direct transmission is impossible. The organism undergoes further development in the body of the fly and within about three weeks the organisms can be transmitted in the saliva of the fly to another mammal. The fly remains infective for the rest of its life, which rarely exceeds six months. The parasite is not transmitted of the pupae. Of all tsetse flies which feed upon infected mammals, only a few, not more than about one in twenty, become infective. The first symptoms of sleeping sickness are fever and enlargement of the lymph nodes, usually of the neck. After about a week the fever diminishes or disappears and the lymph nodes return to normal size, or almost to normal size. There is no definite relation between the size of the lymph nodes and the height of the fever. After a few days or a few weeks these symptoms recur; the fever becomes remittent or intermittent and other lymph nodes enlarge. The lymphoid hyperplasia becomes chronic and variable. During this period the parasites may be found in the blood and in juice extracted from the enlarged lymphoid tissues. These recurrent attacks may persist for months or even for years. After a time invasion of the cerebrospinal fluid, meninges and the brain occurs, and the typical lethargy and mental inertia of sleeping sickness follows. Various convulsive attacks resembling epilepsy may occur; the gait becomes shuffling and uncertain; fine tremors affect the skeletal muscles and the diaphragm, and sometimes the abdominal muscles. Actual sleep may be scanty but apathy is often very profound. Recovery does not occur after the nervous symptoms
appear. During the earlier stages symptomatic recovery is possible. The
periods of intermission can be lengthened and the comfort of the patient
increased by the maintenance of good structural relations of the body,
good hygienic conditions and change of climate.
When recurrent attacks of fever with enlargement of the lymph nodes occurs in an individual who has been in African or in Latin America, the blood and other tissues should be studied carefully in a search for the parasites. Smears made from peripheral blood may show the trypanosomes on the warm stage, as was the case in one of our patients. This is not commonly the case. Thick smears may be made from peripheral blood and this permits them to be found rather more easily. They are easily recognized; the long, slender unicellular organism with its long, slender flagellum and the waving undulant membrane are distinctive. If the organisms are not found in smears from the peripheral blood, about ten to twenty cubic centimeters of blood should be taken from a vein in the elbow into an equal amount of citrate solution. The mixture is then to be centrifuged for five minutes, at a speed of about three hundred revolutions per minute. In the sediment the parasites are easily seen; they accumulate in the leucocyte layer, which lies between the red blood cells and the supernatant plasma. In some cases it is best to take several specimens of ten cubic centimeters each, centrifugalize specimens separately, remove the leucocyte layers, place all together into another centrifuge tube and centrifugalize again. In this manner the organisms from a considerably amount of blood are brought together in a few drops of leucocyte and plasma mixture. In case this method does not demonstrate the parasites, one of the enlarged glands should be punctured, using a sterile and perfectly dry needle. A few drops of fluid from the gland is almost certain to contain the trypanosomes if they are the cause of the symptoms. The blood or the gland extract may be used to inoculate guinea pigs, monkey or rats. The last named rarely succumb to blood inoculation but usually develop great numbers of trypanosomes when inoculated with material from a lymph node which is enlarged. After nervous symptoms occur, the trypanosomes can usually be found in the spinal fluid. They are, very rarely, found in the saliva and the urine of infected human beings. The blood cells show secondary anemia and little
other change. During the fevers there may be slight leucocytosis. The increase
in monocytes, which so commonly occurs in other diseases due to parasites
in the blood, does not occur in trypanosomiasis, at least in any marked
degree. The reticulo-endothelial reactions characteristic of malaria and
kala azar are not noted in this disease. A slight increase in eosinophiles
has been reported.
Trypanosomes have been studied chiefly by means of animal inoculations. The absence of any reaction on the part of the reticulo-endothelial system has been mentioned. Splenectomized animals do not succumb to inoculations more rapidly nor less rapidly than do normal animals, hence the spleen does not seem to be important as a protective agency. Trypanosoma bruccei, T. evansi and T. equiperdum are not pathogenic for human beings but are pathogenic for mice. Rosenthal and others have injected human blood serum into the veins of mice, and then have inoculated them with one of these trypanosomes, whereupon the mice did not succumb to the infection. But if serum from a human with serious liver disease is injected into the veins of the mouse, the inoculation with one of the trypanosomes mentioned causes the usual symptoms and, ultimately, the death of the mouse. Hence it is concluded that the liver produces the trypanocidal substances, whatever it may be. If the mice are injected several times with human serum, the latter loses its protective influence, so that it seems probable that the human serum activates some substance in the juices of the mouse. The serum of human beings does not kill the trypanosomes mentioned, in vitro. Human serum exerts little if any protective influence in splenectomized mice. Other experiments seem to indicate that the spleen produces the substance with which the human serum combines, to protect the mouse against the trypanosomes experimentally inoculated. These and other experiments seem to indicate that there is an indirect relation between the spleen and other areas of the reticulo-endothelial system in protection against trypanosomes, although there is no recognizable direct activity of the endothelial cells in this disease. There is no trypanosomicidal drug which is not even more definitely fatal to the tissues of the host. Patients in the earlier stages should be taken to a temperate or chilly climate, in order to prevent later infections and also in order to avoid transmitting the disease to the carrier insects. Hygienic conditions should be as good as is practicable. Osteopathic treatments which cause a free circulation of the blood through the liver and the spleen are indicated, and any lesions which affect the functions of these organs should be corrected at once. In Brazil, and occasionally in other countries of South America, there is an organism which is sometimes called Trypanosoma cruzi and later called, by Chagas, Schizotrypanum cruzi, which causes repeated fevers in children, and, later, marked enlargement of the thyroid gland. This parasite is carried by several insects of the vicinity, including bedbugs and ticks. These insects and others, live in the cracks of houses. The parasites infect the bugs, and are discharged in great numbers with their feces. The latter are left upon the skin of the human host and gain entrance into the body through wounds in the skin; the wounds caused by scratching are especially dangerous. After a latent period which is probably several years the child suffers from increasingly severe feverish attacks, much pain in the muscles, emaciation and various nervous attacks, the thyroid enlarges, and the further course resembles that of other trypanosome infections. During the acute fever the parasite can be found
in the peripheral blood of the child, but during remissions blood examinations
are futile. Schizotrypanum is about twenty microns long and about one micron
in diameter. It is characterized by a larger parabasal body than is shown
by other trypanosomes infesting the human body. The organisms undergo division
in the voluntary muscles, the brain and spinal cord, and in many glands
of the body, especially the thyroid. With abundant and rapid multiplication
the young organisms form cyst-like structures; these break apart when the
parasites become fairly mature and they then invade the blood. The location
of the cysts determines the symptoms of the disease and accounts for the
varied symptomatology associated with the fevers and thyroid enlargement.
Filariasis is a disease due to the presence of any one of several varieties of filariae in the blood. The most commonly found is Filaria Bancrofti, originally called filarial sanguinis nocturnes. The latter name is due to the fact that the embryos are found in the peripheral blood at night, in persons who sleep at night. They are most abundant at about midnight. In persons who work at night and sleep during the day the embryos are found in the peripheral blood only during the day, being most abundant at about eleven oclock in the morning. There is some reason to believe that this distribution is due to changes in the blood pressure and in the varying amounts of blood in the skin and in the viscera during sleep and wakefulness. Much further study is necessary before the problem can be solved. Filaria Bancroft in the adult form lives in masses, often entwined inextricably. The females are fifty to sixty-six millimeters long and almost or quite two millimeters in diameter; they resemble transparent hairs. The males are forty millimeters or less in length and rarely more than one-tenth millimeter in diameter. The worms are evoviparous. The ova are oval or roundish and have no true shell; they are about fifty microns by about thirty-five microns in size. These are occasionally carried in the blood but being unable to pass the capillaries they occlude the smaller arteries and the arterioles. Normally the ova are retained until they reach the larval stage, the mirofilariae of the peripheral blood. These are variable in length and may be somewhat longer or shorter than three hundred microns; their diameter also varies, but is not far from eight microns, the diameter of a red blood cell. They are able to pass through the capillaries with comparative ease and they are found in the capillary blood taken for an ordinary examination. Having gained entrance into the human body they probably remain indefinitely, undergoing their adult life and their sexual reproductive period in the viscera, especially the lymphatics and the lungs, and their larval period in the circulating blood. The intermediate host is the mosquito; the culex
fatigans is probably the most important. Other species of culex and certain
species of anopheles also act as intermediate hosts. The mosquito bites
the human host, the larval forms are taken into the stomach of the mosquito,
pass into the muscles of the mosquito, undergo further development, and
finally reach skin of another human being through the bite of the mosquito.
Probably a very long time is required for development within the human
host, for children show no symptoms of disease until they are five or ten
years old, in countries in which filariae are abundant. The development
within the body of the mosquito probably requires less than a month.
These worms may infest the human body for years without causing any noteworthy symptoms. The worms have been demonstrated in the blood of about one in four of the natives in certain countries and many of these persons seemed to be in ordinarily good health. Chyluria or hematochyluria is usually the first symptom. The urine, usually otherwise normal, contains abundant fine fatty globules and this causes it to resemble a milky fluid, which may be pinkish from blood. On settling a reddish clot is sometimes noted; this is composed of blood. This condition may be present at intervals, or almost or quite constantly, and very often no other symptoms occur for many years. In one of our cases this was the sole symptom during the time the patient was under observation, about two years. Occasionally the clots are formed in the bladder and this may cause difficulty in urination. The worms or the parasites are not often found in urine, but the blood should be carefully examined at different times of the day and the night until the microfilariae are found. It must be remembered that Chyluria may occur, though rarely, because of other etiological conditions. Elephantiasis is commonly associated with Filariasis,
though it may never occur. The legs, scrotum, labia and, rarely, other
parts of the body undergo progressive increase in size, sometimes becoming
enormous. The enlargement may be gradual or may be sudden, and in this
case is usually associated with fever.
The finding of the worm in the peripheral blood is the most definite method of diagnosis. It may be found on making an ordinary blood examination when its presence has not been suspected When it is suspected a thick smear should first be made and this examined with one-sixth objective; even a two-thirds objective with a one-inch or a half-inch eye-piece may be sufficient to allow them to be seen. They are noticed at first because of the turmoil of the red blood cells on the warm stage; these are whirled about by the lashing movements of the filaria. Smears may be dried and stained with thionin or hematoxylin for permanent use. If the worms are not found in such a specimen the blood should be centrifuged. Take about one cubic centimeter of blood into a centrifuge tube containing about nine cubic centimeters of two per cent acetic acid. Mix thoroughly and centrifuge for about five minutes at about five hundred revolutions per minute. The red blood cells are destroyed by the acetic acid and the debris of these, with the worms and the white cells, are thrown down. Take a drop of this sediment and examine as before. This test may be repeated at several different times of day and night if necessary. The filaria are more easily found in capillary than
in venous blood. A fairly deep puncture is necessary in order to secure
the rather large amount of blood. There is no harm in using antiseptics
which dilate the blood vessels of the skin, in this test, and fairly vigorous
rubbing of the skin may increase the number of embryos present.
PLATE XI
The blood shows moderate eosinophilia in practically
all cases. Moderate degrees of secondary anemia are common. The actual
and differential counts are otherwise almost or quite normal.
Sanitary measures are important. Mosquitoes should be exterminated Infected persons should be protected against mosquito bites. In countries in which filariae are present, all persons should be guarded against mosquitoes. There is no adequate treatment for the disease. Any drug which exerts even a detrimental effect upon the worms injures the host more seriously. Limiting the fats of foods diminishes or prevents chyluria and hematuria. In this way the discomfort associated with the passing of blood clots through the urethra is lessened or removed. All measures which increase the nutrition and the
general health of the patient should be employed. Since the manner in which
the body protects itself against the worms is not known (if, indeed, there
is any protection at all) it is impossible to say whether the maintenance
of a good circulation of the blood has any parasiticidal effects or not.
Certainly the maintenance of good nutrition and good circulation enables
the patient to live more comfortably and efficiently than he could do otherwise.
Several forms of spirochetes, spirosomes or spirilla are known to cause diseases. Most of these are filth disease, so-called because they are transmitted from one person to another through the intervention of lice, bedbugs, ticks, or other insects whose presence indicates lack of cleanliness in persons or in dwellings. Some species are transmitted directly from one diseased person to another and others are carried by mosquitoes. Methods of transmission differ for different species. The biological place of these organisms is still somewhat in dispute. Schaudinn and others place them with the protozoa; Dobell and many others class them with the bacteria, while Doflein and many others beg the question by forming a separate class for organisms which are intermediate between protozoa and bacteria. However puzzling the question of classification may be, there is no question about the facts of the life history and the pathogenicity of these organisms. There are very many spiral-like organisms which infect
lower animals but only comparatively few which infect man, and of these
not every species, and not every infection of pathogenic species, causes
recognizable symptoms of disease. This lack of pathogenicity does not seem
to depend upon the development of parasiticidal factors in the human body,
as is the case with certain pathogenic bacteria, but rather on a passive
non-resistance on the part of the cells of the body of the host. This reaction,
or, rather, lack of reaction, is one factor which suggests that the biochemical
relations of these parasites are with the protozoa rather than the bacteria.
There are other factors concerned, however, and the entire question of
classification must await further study of these interesting and dangerous
organisms.
This is a general term which includes several related diseases, all due to some spirochetal infection and all associated, directly or indirectly, with filthy habits, filthy surroundings and, usually extreme poverty. European relapsing fever has for its specific infectious agent the spirochete obermeieri (spirosoma obermeieri; spirillum obermeieri; borellia recurrentis; spirosoma recurrens. This spirillum varies from about ten to about fifty microns in length and rarely exceeds half a micron in diameter. It has from four to sixteen turns and is flagellated. The ends are sharply pointed. It is freely motile during the early stages of the fever, then diminishes in motility until only the barest waving is perceptible. It reaches its greatest abundant in the peripheral blood just before the crisis in the fever, and during defervescence it may be difficult to find any specimens in the peripheral blood. During intermissions it is almost impossible to find any specimens though of the spirochetes to appear in the monkeys peripheral blood within a few days to a week. If death occurs during an intermission, the spleen
and bone marrow show hyperplasia and the organisms are abundant in these
tissues as well as in other lymphoid tissues and in the liver, kidneys
and other glandular viscera.
The disease is characterized by repeated attacks of high fever lasting about a week. Nausea, vomiting, profuse sweating, and convulsions and other nervous symptoms may be extremely severe. Intermissions last ten days to several weeks. Later attacks of fever may be less and less severe until recovery seems complete, or more and more severe until death results, usually from exhaustion or from intercurrent disease which may itself be apparently negligible. Death from relapsing fever is hardly to be expected except in unusually severe cases, but recovery is long delayed, convalescence slow and often interrupted, and even for many months after apparent recovery other attacks may occur. The organisms are best recognized in rather thick warm slide preparations of peripheral blood, and these must be made during the early stages of the fever. They move very freely among the red blood cells, which themselves are not disturbed by the moving spirilla. Later in the fever the spirilla become less and less motile and it may be necessary to make stained smears in order to find them. Dark stage illumination is best. They may be very abundant during the early stages of the fever, so that in a thick smear observed under the one-sixth objective as many as twenty or more may be found in a single field. They may be absent or scanty on the first day of the fever, and they increase until just before the crisis, when they begin to diminish in numbers rather rapidly. They may form ring-like bodies during defervescence, and at all times, even during intermission, there may e abundant small highly refractive bodies in the blood which may be degenerative fragments of the parasites or may be spore-like structures. The blood cells show the characteristics of secondary anemia. Leucocyte counts are usually high, but rarely exceed 15,000 per cubic millimeter. Large hyaline cells and eosinophiles are increased moderately. This eosinophilia suggests protozoal rather than bacterial infection. Neutrophiles and large hyaline cells may contain fragments of the spirilla, and in this relation the spirilla resemble bacteria rather than protozoa. The urinary changes suggest the renal complications always present in this, as in other high fevers. In extremely severe cases acute hemorrhagic nephritis may be present. These are the blackwater cases so feared in countries in which the disease is endemic. Several varieties of relapsing fever occur in different countries. Spirilla obermeieri causes the European type of relapsing fever and this has just been described. It seems to be carried especially by bedbugs, though other insects seem also to act as intermediate hosts. Spirosoma or spirillum duttoni (Borrelia duttonia) causes the relapsing fevers of East Africa and West Africa. It is transmitted by ticks (Ornithodorus savignyi or O. moubata). The tick becomes infected by sucking human blood containing the parasites, and it transmits the infection to its young. The coxal fluid of the tick and the feces contain the parasites and this mixture is left upon the skin of the human being next bitten by the tick. This material as well as the biting of the tick causes itching of the skin. On scratching the tick may be crushed upon the skin, and both the remnants of the tick and the mixture of coxal and fecal material are apt to be rubbed into the skin through the abrasions due to the scratching. Spirosoma (or spirillum or borrelia) carteri causes the relapsing fever of India. It is thought to be transmitted chiefly by lice, and either the pediculus capitis or the P. vestimenti may carry these organisms. S. persica causes the Persian relapsing fever. It is carried by ticks, for the most part. The relapsing fever of Northern Africa is caused by S. berberi or Borelia berberi. It also is transmitted by lice. S. novyi has been found in the United States and it caused a severe epidemic in several large eastern cities during the middle of the eighteenth century. It is about ten microns long and has two or three rather sharp turns. It is not now found in the United States. There is a form of relapsing fever in Panama which is carried by ticks. The elimination of the disease depends upon sanitation, and with cleanliness and the destruction of lice, bedbugs and ticks the disease soon disappears. During the fevers the osteopathic treatments which control the circulation of the blood through the viscera are usually effective. The convulsions and other nervous phenomena are sometimes prevented by relaxation of the abnormally tense cervical tissues and the correction of lesions of the cervical vertebrae. Patients who do not have such lesions rarely show any nervous symptoms. The nausea and vomiting should not be treated until the stomach has been well emptied; after that if the vomiting persists inhibition of the upper splanchnic centers is all that is needed in most cases. There is no adequate parasiticidal drug. Recovery depends upon the action of the normal parasiticidal activities of the body and upon the prevention of re-infection. Change of climate is advisable in order to avoid re-infection and to promote the recuperative powers of the body as a whole. Records of the osteopathic treatment of the disease are scanty and are limited to those cases which have come to the United States from other countries. In all these cases there have been complicating factors so that typical cases have not been well studied. There are several other spiral-like organisms which infect the human body and may occasionally be found in the blood. Leptospira icterohemorrhagica (spirochete icterohemorrhagica) is not ordinarily found in the blood on direct examination, but it can be successfully inoculated into guinea pigs from the blood of the patient or from his urine. This parasite causes infectious jaundice (Weils disease). It is carried constantly by wild rats, in countries in which this form of jaundice is endemic, and human beings become infected by drinking water polluted by the urine of the rats, or by eating uncooked vegetables grown in ground polluted by the rats, or by some other accidental means. This spirochete is rarely more than fourteen microns in length and one-fourth micron in diameter. It stains a reddish or purplish color with Giemsas stain but it does not take any of the ordinary aniline stains. Leptospira icteroides (spirochete icteroides) causes yellow fever. It is transmitted by the mosquito, stegomyia fasciata. This insect becomes infectious about twelve days after it has bitten a human being during the first few days after the onset of an attack of yellow fever. The mosquito is an intermediate host. Leptospira icteroides rarely exceeds nine microns in length or one-fifth micron in diameter. It is sometimes visible by dark-field examination of fresh blood but does not stain readily. It can be cultivated or animals can be successfully inoculated form the patients blood. Leptospira hebdomadis causes a seven day fever in Japan. Wild mice carry the organism, and human beings are infected from the water and the ground polluted by the mice. Leptospira morsus-muris causes rat-bite fever, which follows the bite of an infected rat. It is of relapsing type and resembles the ordinary form of that disease in many respects. It occurs only in Japan. Spirochete pallida (treponema pallidum) is the cause of syphilis. It is rarely found in the blood, and blood cell examinations are not commonly employed for its diagnosis. The Wassermann test and the Kahn test are the most common diagnostic methods. In syphilis the blood picture includes moderate eosinophilia with moderate lymphemia. Leucocytosis and the usual findings in secondary anemia occur under certain circumstances in syphilis. Many other forms of spirochetae, spirilla, treponemata, and similar organisms are occasionally found associated with various ulcers and sores of the skin; they are often found in the healthy as well as in the diseased mouth, and harmless forms are isolated from many specimens of water and from the bodies of animals. Leishmania are parasites found in the blood and in the tissues during the progress of certain diseases. The organisms appear to be alike, but different strains or varieties causes different forms of disease. The organisms are usually flagellated in cultures and in the invertebrate hosts, but are usually non-flagellated in the mammalian host. In the human host and in the canine host the Leishmanias are found within the large hyaline phagocytes of the blood and in the spleen and other lymphoid tissues. The reticulo-endothelial system seems to be eof great importance in protecting the body against theses organisms, as is the case with malarial infections. The organisms may divide rapidly within the phagocytic cells, and finally the cell resembles a small cyst, filled with the parasites. In other instances the parasites are digested and absorbed by the phagocytic cells, and it is in this way that the further injury due to the organisms is prevented. The organisms are also very abundant in the red bone marrow and in granulation tissue around the lesions caused by the Leishmanias. In their mammalian hosts Leishmanias are about a four microns long by about one and one-half microns in diameter. Somewhat larger and somewhat smaller forms may be found. Each cell contains an oval, round or roundish nucleus placed at about the center of the cell. There is a round karyosome associated with the nucleus. The nucleus stains avidly with ordinary nuclear dyes. Near the periphery there is a parabasal body or centrosome which takes nuclear stains quite deeply. The long axis of the parabasal body lies at right angles to the long axis of the cell. The blood shows the usual findings of secondary anemia, except that leucopenia is frequent. The leucocyte count rarely exceeds three thousand cells per cubic millimeter and is often less than two thousand. The neutrophiles are both relatively and absolutely diminished and the large hyaline cells both absolutely and relatively increased. Lymphemia may be quite marked. The parasite is not often found in the blood on ordinary examinations and some method of concentrating the parasites is necessary. For demonstrating the organisms take several cubic centimeters of venous blood into a centrifuge tube containing an equal amount of five per cent potassium oxalate, and centrifuge at about five hundred revolutions per minute for six minutes. The red cells are then at the bottom of the centrifuge tube, the plasma at the top, while the white cells form a thin layer at the top of the red cell column. Smears made from the white cell layer contain great numbers of leucocytes and the parasite is occasionally found within the large hyaline cells or in rather large masses resembling zooglea. They are best stained with one of the methylene-blue-cosin blood stains. If the parasites are not found after several attempts have been made to find them in concentrated blood, puncture of the spleen or the liver, the removal of a small bit of a rib, or the removal of one of the enlarged lymph nodes, may be considered. All of these methods are somewhat dangerous, and fatal hemorrhages occasionally follow such operations. Smears made from the granulation tissue or from the firm base of the local sore usually contain the organism in great numbers. The symptoms are characteristic; a series of irregular attacks of fever is soon followed by enlargement of the spleen and sometimes the lymph nodes of the neck and elsewhere, and by progressive anemia and emaciation. Recovery is doubtful but the patient may live for many years. Two cases have been examined in our laboratories. In one the diagnosis was fairly certain from the history and the symptoms. The parasites were not found in the blood, and no attempt was made to secure extracts from the liver, spleen, lymph nodes or marrow. The patient disappeared and his death was reported two years later. In another case the diagnosis was not suspected before death. Microscopic examination of the spleen after death disclosed great numbers of Leishman-Donovan bodies. Leishmania infantum was first found in Naples and Rome, and since then has been found in Tunis, Malta, Sicily, Egypt, Turkey, Arabia and other countries bordering the Mediterranean. Children and dogs are chiefly affected, and the disease is probably carried form one to the other, and perhaps from one child to another, by fleas. Leishmania tropica causes the Delhi boil, also known by many other names. It was first found in Oriental countries, especially India, Persia, Arabia and other tropical countries; later it was found in Egypt and other countries of Northern Africa, and in several Mediterranean islands. The disease called espundia, in Brazil and other countries in Latin America, is probably the same disease. No treatment has been found successful. Methods which increase nutrition, enforce cleanliness and freedom from insect parasites and which encourage good circulation blood through all the body are indicated. Antiseptic washes and comfortable dressings should be used for the local lesions on the skin. |
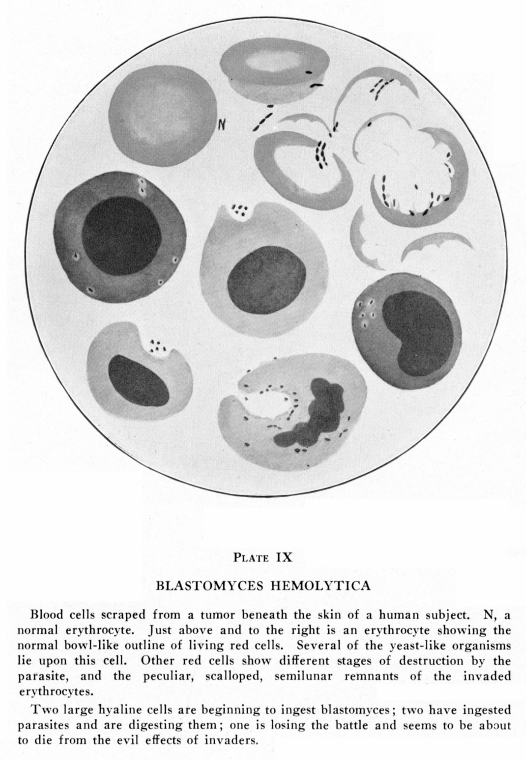{kind=link}
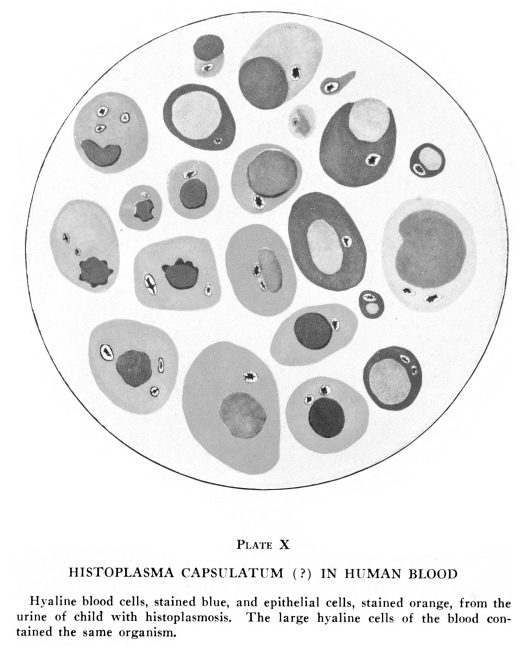{kind=link}
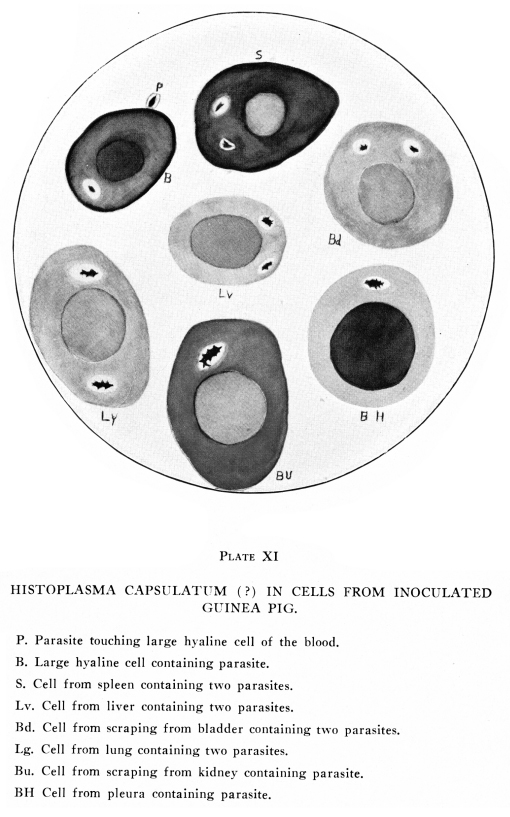{kind=link}