
| Blood-forming tissues depend upon other tissues of the body for nutrition, removal of katabolites, nerve impulses and probably certain hormones. Without the various influences derived from normal activities of other tissues of the body the hematopoietic tissues become unable to produce normal blood. In this respect the bone marrow, spleen and other tissues concerned in the metabolism of the blood cells and plasma share in the mutual dependence which is shown by all parts of living metazoa. Secondary anemia is, as the term indicates, an impoverishment of the blood due to some recognizable cause. The term is commonly applied to deficiency of hemoglobin, whether this is due to a lack of red cells or to a lack of hemoglobin within the red cells. Secondary anemia may be due to any one or more of a long number of causes, and its characteristics vary according to the etiological factors. The symptoms are not very definite
and are often masked by the symptoms due to the cause of the anemia.
Palpitation, pallor, dyspnea, malaise, vague headaches, weakness,
insomnia and excessive fatigability are common. Edema of the feet
and legs, loss of appetite, petechial hemorrhages of the skin
or mucous membranes, epistaxis, retinal and uterine hemorrhages
occur rather frequently. The pallor is often masked by excessive
dilatation of the arterioles of the face, which gives a ruddy
tint to the cheeks, especially. In certain cases sallowness or
mild jaundice mask the pallor. CHARACTER OF BLOOD CELLS IN SECONDARY ANEMIA
Secondary anemia is associated
with a typical blood picture though this may be somewhat modified
as a result of varying individual reactions to disease or varying
pathogenetic influences. The typical blood picture in secondary
anemia shows little or no diminution in the number of red cells
but the hemoglobin is considerably reduced, usually to less than
70% of the normal for the individual. The color index is low, usually
less than 0.7 and often being below 0.4. The resistance of the red
cells to saponin solutions is increased. The platelets vary but
are usually diminished to half the normal number, or even less.
The white cells are often increased, and the differential count
as well as the actual leucocyte count very often indicates the nature
of the primary disease. The blood volume may or may not be affected;
this depends upon the cause of the anemia. The relations between
cell volume and plasma volume also show variations in certain cases.
Fibrin threads are scanty and slowly formed. Viscidity, specific
gravity and usually osmotic tension are low. Rouleaux are subnormal
and are slowly formed. Other factors vary with the nature of the
primary disease causing the anemia.
Anemia is universally present as a result of diseases which affect the blood-forming tissues. All vertebrates which are subject to nutritional, developmental, toxic or parasitic diseases are subject also to secondary anemias. The blood changes are similar, varying only according to the varying types of blood cells found in different groups of animals. The manner in which the organs of the body react to causes of anemia varies for different animal groups also. In the lower mammals, in birds and in reptiles extra-medullary hematopoiesis is abundant after hemorrhages. Instead of neutrophilic leucocytosis many of the lower animals show mononucleosis or lymphemia. Increase in the eosinophiles occurs in certain birds, after infections. Wild birds and mammals in captivity suffer from
secondary anemia due to parasitic infections, osteomalacia, gastrointestinal
inflammations of various etiology, nephritis and other conditions
which cause anemia in human subjects. The severe secondary anemia
of kittens infested with fleas is very common. In the treatment of patients with secondary anemia the most important factor is, of course, the removal of the cause of the anemia when this is possible. After the removal of cause, and in those cases in which the cause of the anemia is beyond control, it is necessary to secure the most adequate possible renewal of the blood cells and the hemoglobin. For this the first and most important requisite is to secure correct structural relations of the body and all its parts. Since new blood cells are developed in the red bone marrow it is essential that the bones have good circulation of good blood, and unimpeded nerve pathways to and from the central nervous system. Since the ribs contain so great a proportion of the hematopoietic areas these must receive especially careful attention. The thorax must be kept flexible and the movements of the ribs in breathing must be free and as extensive as is practicable. Rib lesions must be corrected and the patient taught to breathe properly, if he is not already using correct respiratory movements. The skull, innominates, scapular and other flat bones, the vertebrae and the short bones of the bone also contain fairly extensive areas of red bone marrow, and lesions affecting these should be corrected. Since the cells of the liver and the spleen play an important part in the metabolism of hemoglobin and blood cells, these organs must be kept as nearly in normal condition as possible. Lesions of the ninth thoracic vertebra affect the spleen, especially, and lesions of the tenth thoracic vertebra affect the liver; lesions of adjacent vertebrae and ribs also affect these organs and such lesions may prevent the best possible restoration of the blood after the cause of the anemia has been removed, or they may prevent adequate reaction to persistent causes of anemia which are essentially not serious in pathogenesis. Other tissues may be important in the control
of the hematopoietic organs, and anything in the body which interferes
with the general health should receive attention. But the most important
factors by far, in dealing with the secondary anemias, is, first
the removal of the cause of the anemia when this is practicable,
and second the osteopathic treatment of all incorrect structural
conditions which might prevent adequate functions of the red bone
marrow, the spleen and the liver. After this attention should be
given to incorrect structural relations of the other tissues of
the body, and to any unhygienic conditions that may be found. The
diet should receive attention, though any ordinarily wholesome and
varied meals provide all that is necessary for the manufacture of
good blood. Much experimental study has been given to the place of various therapeutic agents in hastening recovery from anemia. In these experiments a group of animals is made anemic by repeated or single bleedings, by the administration of hemolytic drugs, or by the omission of iron or of some other necessary factor for the manufacture of hemoglobin. Animals thus made anemic are then divided into smaller groups, and each group is then given special diets, drugs or other therapeutic measures and the speed with which hemoglobin is regenerated in the animals is considered a measure of the potency of the therapy under consideration. Classical medicines have received much attention. The administration of iron in inorganic form has been studied with especial care. In animals with moderate anemia the giving of inorganic iron does not seem to facilitate regeneration of hemoglobin efficiently but the giving of foods rich in iron in the organic form, especially in connection with foods containing the piperidin ring, greatly encourages the formation of new hemoglobin. Those foods containing molecules closely resembling hemoglobin have been found best adapted to the formation of new blood in nearly all the animals tested. Lean meat, liver, sweet-breads and other glandular viscera, and blood itself all provide the best foods for promoting hemoglobin regeneration. Vegetable foods containing chlorophyll and chromophyll are also useful. It must be remembered that other elements than iron are important in hemocytopoiesis. Dried apricots, peaches and other fruits have been found useful in the regeneration of anemic animals and in the diet of anemic human beings. The exclusive milk diet has been found useful in selected cases of secondary anemia and in chlorosis. It cannot be employed permanently for obvious reasons. The value of an exclusive milk diet for a few weeks seems to lie in the fact that milk provides an abundance of easily digested and easily absorbed proteins. Indirectly the fact that large amounts of fluid are thus given may be important in dietetic therapy. An exclusive milk diet for too long a period of time causes an anemia of persistent type. In one of our cases a child of two years became anemic because he suddenly refused any food except milk after he had been on a normal mixed diet for nearly a year. In this case no cause for the sudden aversion for ordinary foods could be explained, except that a fall had produced a lesion of the fifth to the seventh thoracic vertebra. The strength and weight diminished considerably after the accident. The correction of these lesions improved nutrition slightly but the abnormal appetite persisted. Finally he was given no milk during the daytime and was starved into eating proper foods within about four days. During this time milk was given him at bedtime and in this way he was able to sleep normally and to maintain reasonable strength. Within a week he was taking normal foods and he soon regained his normal weight and strength. After fifteen years he is robust and normal. There is still more than an average appetite for milk, though no abnormal aversion for other foods is recognizable. Many authors have found that the administration of inorganic iron in any considerable amounts depresses the hematopoietic tissues and thus delays recovery from these experimental anemias. Inorganic iron has been found to be utilized
in the regeneration of hemoglobin in extremely severe experimental
anemias. After several generations on completely iron-free diets
certain laboratory animals become extremely anemic though they retain
life and even continue to breed. If some soluble inorganic iron
is then added to their original iron-free diets, these animals develop
hemoglobin and finally show almost normal blood. After extremely
severe anemia has been produced in other animals by prolonged and
repeated bleedings, together with the use of an iron-free diet,
the animals seem to utilize some inorganic iron in regenerating
blood. The possibility that inorganic iron, administered under extremely
unusual experimental conditions, can be utilized in the regeneration
of hemoglobin seems certain. That inorganic iron has a really useful
place in the treatment of the secondary anemias seems extremely
doubtful. There is no question at all that the iron which is in
combination with the other molecules and radicles which go to the
formation of the hemoglobin molecule is by far the best food for
persons with secondary anemia. Diet which is chiefly carbohydrate fails to facilitate regeneration of blood. Starving animals regenerate blood more rapidly than do animals on a high carbohydrate diet. This is, of course, due to the fact that starving animals are really on a meat diet. Animals which have undergone splenectomy regenerate hemoglobin as rapidly, but not more rapidly, than do animals with normal spleens. Animals in high altitudes are made anemic with greater difficulty than are animals near the sea level, whether the anemia is produced by repeated bleedings or by the administration of hemolytic drugs. Animals regenerate hemoglobin more rapidly in high altitudes. Experimental animals made anemic in any manner
regenerate blood and hemoglobin more rapidly in sunlight or under
the influence of ultra-violet rays than in darkness. This seems
to be due to the effects of sunlight on metabolism directly. Animals
which have lived in darkness for many generations have normal hemoglobin.
A classification based upon causes of the anemia plus the effects produced upon the blood cells is helpful in diagnosis. Secondary anemias may be classified primarily as nutritional, hemorrhagic, developmental, toxic and parasitic. Any given case may be due to the effects of two or more of these causes but it is possible in nearly every case to determine some one factor in etiology which is of most practical importance. For example, that individual who has a developmental imperfection affecting the blood-forming tissues is more easily affected by disturbed nutrition than is one whose structural relations are normal. In such a case the nutritional disturbance alone can be successfully treated, though the developmental cause may be of greatest importance so far as etiology is concerned. Serious developmental anemias are usually called primary anemias. Each group presents certain factors of resemblance
and the information gained from a study of the blood cells is useful
in diagnosis and in determining the most efficient methods of treatment.
In the anemias called nutritional the essential factor is the lack of a sufficient supply of food for the hematopoietic tissues. Many factors are concerned in providing the bone marrow and the lymphoid tissues with proper nutrition and a failure of any one of these factors may cause anemia. When an insufficient amount of food is eaten,
the bone marrow maintains its nutrition and circulation long after
the bone marrow maintains its nutrition and circulation long after
the other tissues of the body show serious effects of starvation.
The most common dietetic defect concerned in anemia is a lack of
food containing the globulins from which hemoglobin can be synthesized.
Only an extremely restricted diet fails to provide enough iron and
other inorganic salts to meet the daily requirements, for this amount
is very small. But the requirements for globulin are considerable,
and there is no provision made for preserving the globulins for
further use. It will be remembered that the iron-containing moiety
of hemoglobin is saved to be used again while the iron-free pigment
is excreted from the body after some stay in the plasma. The globin
part of the molecule is probably used as food for other tissues,
but it is not known to be preserved as far as the formation of new
blood is concerned. The supply of the globulins and other proteins
in the food must be adequate and must be steadily maintained if
anemia of the nutritional type is to be prevented. The anemia due to a lack of proper food intake presents certain definite and usually recognizable peculiarities. The red cells are present in almost or quite normal number but the hemoglobin is considerably diminished. In fifty cases of partial starvation associated with reducing diets the red cell counts varied between 4,200,000 and 5,400,000 per cubic millimeter; hemoglobin between 40% and 86% of the normal for the age and sex of the patient; color index between 0.45 and 0.78. In all these cases the food intake had been kept extremely low and in all cases acidosis had been prevented by the use of very large amounts of citrus fruits, baking soda or magnesia. Weight reduction in these cases was severe, varying from sixty pounds in two months for a very fat man to five pounds in one month for a woman already emaciated. There was no known organic disease in any of these patients before the beginning of the weight-reduction, and in fifteen cases there had been a fairly careful physical examination with ordinary laboratory tests, before the special diets for the reduction of weight had been begun. In the other cases the patients themselves had carried on the diet with no professional advice. The changes in red cell count and hemoglobin given above are characteristic of anemia due to partial starvation. In such cases the white cells show characteristic
changes. The granular cells are diminished both absolutely and relatively.
The leucocyte count varies between 3,000 and 4,500 in typical cases,
with the neutrophiles between 40% and 55%. Small hyaline cells are
relatively increased but the actual numbers remain almost or quite
unchanged. The large hyaline cells show a slight increase both relatively
and actually. The eosinophiles are unaffected actually in those
cases in which the protein intake remains fairly adequate. If the
protein intake is too low the patient is on a high meat diet (his
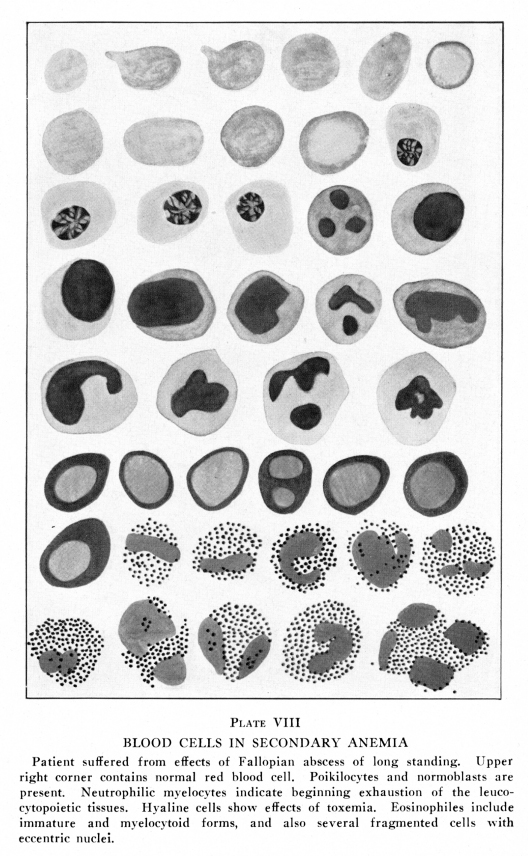
own muscles) and the eosinophiles are somewhat increased. Myelocytoid
and immature forms are present in moderate numbers. (Plate VIII)
PLATE VIII Patient suffered from effects of Fallopian abscess of long standing. Upper right corner contains normal red blood cell. Poikilocytes and Normoblasts are present. Neutrophilic myelocytes indicate beginning exhaustion of the leucocytopoietic tissues. Hyaline cells show effects of toxemia. Eosinophiles include immature and myelocytoid forms, and also several fragmented cells with eccentric nuclei. If the special diet includes too small an amount of water intake the blood may be concentrated and the red cell count then exceeds the normal number while the hemoglobin remains at about the normal amount or is only slightly reduced. The white cells show an increase, sometimes to 12,000 per cubic millimeter. The lack of water is associated with toxic symptoms and there is neutrophilic leucocytosis. The hyaline cells may show a slight actual increase in this condition; they do not show relative increase when the toxemia is recognizable. If the special reducing diet is based on scanty
proteins and there is no provision for voiding acidosis, the red
cells are often above normal in number with very low hemoglobin.
Three such cases are recorded. The diet included only one slice
of thin, white toast without butter, three cups of water or weak
tea with sugar but no milk or cream at each meal and an allowance
of one ounce of hard candy during the day, to be eaten when desired.
This diet was to be used for ten days, then the subject was allowed
a day of food ad limitum. In each of these cases the red blood cells
exceeded 5,000,000 with hemoglobin below 50% of the normal for the
individual. Toxic symptoms and acidosis were marked. The granular
cells were 1,400 per cubic millimeter and the hyaline cells above
4,000 per cubic millimeter in each case. In all three cases the
water intake was insufficient for physiological requirements. The
loss of weight was negligible in one case, and in the other cases
was twenty pounds in two months for a fat woman, and five pounds
in three months for a lady already rather thin. The fat lady became
diabetic within six months; whether the starvation diet had any
etiological significance is unknown. Absolute starvation and complete fasting affect the blood less severely. The toxemia associated with complete fasting causes a moderate neutrophilic leucocytosis. With complete starvation or complete fasting the subject utilizes his own body to meet physiological requirements. After a few days of using the glycogen of the liver and muscles and a few days of fat feeding the muscles begin to be used as food and the patient is on a high meat diet. The blood cells are about normal in size, hemoglobin content and numbers. The white cells show the effects of toxemia, due to the high meat diet and the fact that the excretory organs are usually somewhat inactive under these conditions. The leucocytes show markedly increased activity on the warm slide and they usually begin to die within fifteen minutes. The eosinophiles show especially rapid motion. Fibrin is formed within two or three minutes during the time the muscles are being used as food and the threads are fine, short, of irregular contour and often arranged in radiating star-like groups or in an irregular net work of somewhat vaguely formed meshes. Fibrinolysis is normal in about three-quarters of all cases until the wasting of muscles has become extreme. An undifferentiated proteolytic ferment is found in the blood of many patients during rapid wasting of muscle tissues, and this masks fibrinolysis because it digests fibrin as well as cells in less time than is required for normal fibrinolysis. During the days of high fat feeding, in complete
starvation, there are fine dust-like globules of fat in the plasma
and the hyaline cells often contain small globules of fat. The fat
globules are found in the blood after all evidence of heavy fat
feeding disappear, and they are probably derived from the disintegrating
muscles of the body. This is not certain, because even after death
from starvation some fat remains in the body. Diets proportionately too high in carbohydrates cause moderate secondary anemia with moderate neutrophilic leucopenia. The hyaline cells are relataively high and are often absolutely moderately increased. The blood plasma is paler than normal. Bile pigments are not present in these cases unless there is an associated disturbance in the circulation through the liver. Diets proportionately too high in proteins show the effects of moderate toxemia of the type associated with abnormal protein katabolism. Neutrophilic leucocytosis is moderate, rarely exceeding 9,500 cells per cubic millimeter in typical cases. The neutrophiles show the effects characteristic of intestinal toxemia but the findings are less pronounced; basophiles and eosinophiles show moderate increase. Red cells and hemoglobin are normal or only slightly diminished. The color index is never very low and usually remains at about unity. Diets proportionately too high in fats are usually associated with moderate secondary anemia with a low color index. These diets, when habitual, are nearly always associated with some evidence of hepatic disorder and bile pigments are often found in the blood plasma. The white cells show marked evidences of the effects of cholemia. Diets which include too high an amount of colored
vegetables frequently cause carotinemia. Persons with renal disorders
or with lesions of the eleventh and tenth thoracic vertebrae are
especially apt to show this discoloration of the plasma with carotin.
The white cells show the effects of moderate toxemia, usually of
the fatigue type. The red cells and the hemoglobin are normal or
only slightly decreased. The color index does not vary far from
unity in typical cases. Starvation may occur if an adequate and correct diet is provided but indigestion and absorption are inadequate. In stenosis of the esophagus the food cannot be properly ingested. It sometimes occurs that sufficient food is swallowed but with such difficulty that digestion is disturbed and starvation is much more serious than can be accounted for on the basis of the actual food intake. Anemia is of the starvation type. In gastric ulcer the quality of the blood changes depends upon the amount of hemorrhage. With hyperchlorhydria a moderate increase in the alkalinity of the blood is suggested by a slightly increased basophilia of the leucocytes, most noticeable in the hyaline cells. A well developed ulcer is associated with an increase in the mast cells and Turck cells are frequently found. The eosinophiles are slightly increased. Red cells may be diminished, rarely below 80% of the normal for the individual affected. Hemoglobin shows greater reduction, usually below 75% of the normal for the individual. The color index rarely exceeds 0.7 in cases without hemorrhage. Cases not associated with tendency to cancer show normal fibrinolysis and normal fibrin development on the warm slide. The leucocytes show normal activity and live well on the warm slide. The occasional relation of cancer and ulcer is significant. Fibrinolysis is absent in about twenty-five per cent of all human beings, who thus lack at least one cancer-protective factor. In terms of the fibrinolysis hypothesis, these individuals would be especially prone to develop cancer at the site of an ulcer in the stomach. Surgical intervention should be considered when gastric ulcer is found in persons with absent or deficient fibrinolysis. Gastric cancer is associated with the blood changes noted in other forms of malignancy. If hemorrhage is considerable the blood often assumes the characteristics of pernicious anemia. The red cells and the hemoglobin are reduced in approximately equal proportions in most cases. Gastric cancer shows a greater tendency to the development of undifferentiated proteolysis than is noted in other forms of cancer, and in quite early cases of cancer of the stomach the diagnosis may be suggested by the presence of this ferment in the blood. Eosinophiles are slightly increased and eosinophilic myelocytes are more abundant than in other forms of cancer. With invasion of the red bone marrow by the metastases from cancer of the stomach myelocytes increase steadily in numbers in the circulating blood. Cancer cells undergoing abnormal karyokinesis are found, though very rarely, in the blood of patients with wide-spread metastases in the bone marrow. Fibrin is formed abundantly and speedily on the warm slide. The threads are long, heavy, irregular in content or definitely beaded, often arranged in radiating or net-like masses and often containing highly refractile particles entangled in the fibrin threads. Gastric atony due to lesions of the seventh thoracic or of adjacent vertebrae is often associated with abnormal hunger and thus with habitual overeating or overdrinking, or both. The passage of the food through the stomach is slow. Hypochlorhydria is a very common associated condition. Fermentation often occurs in the stomach. Proteins are not acted upon properly by gastric juice of subnormal acidity and intestinal putrefaction is thereby facilitated. Intestinal flora are affected; the putrefactive bacteria increase much more rapidly than do the fermentative bacteria. Various abnormal products of fermentation, putrefaction and imperfect digestion are absorbed into the blood stream. Achlorhydria is often a congenital defect. In such cases the blood cells include a few immature or reversionary types. The evidences of nutritional anemia are then superimposed upon a developmental type of anemia. If the food of these patients consists of excessive carbohydrates, the toxemia associated with the secondary anemia is characterized by low fibrinogen content of the plasma, delayed fibrin formation on the warm slide, increased eosinophilia of the blood cells, increased lymphocyte count, subnormal hemoglobin content with almost or quite normal red cell count and a low color index. The nuclei of the granular cells are less basophilic than in normal blood, the nuclei have frayed or ragged edges. The nuclei of all the leucocytes are somewhat swollen, show no pseudopod-like projections and their chromatin masses are indistinct. If the diet includes an excess of protein foods the leucocytes show atony, the apparent diminution of alkalinity is still more marked. Cholemia is common in such a condition. Fine, dust-like globules of fats are often found in the blood plasma and within the hyaline cells. If the diet include an excess of protein foods
the leucocytes show pronounced evidences of toxemia of the type
associated with abnormal protein katabolism. Fibrin appears quickly
on the warm slide and the threads are heavy, irregular in contour,
often beaded, and often arranged in an irregular network of indistinct
fibers. Refractile bodies are abundant and these usually include
iodophilic, Sudanophilic and unstained particles. The nuclei are
irregular in shape but not often frayed; projections of nuclear
substance into the protoplasm, often resembling pseudopodia, are
abundant in the nuclei of neutrophiles. Abnormal conditions affecting the intestinal tract cause different conditions according to the nature of the disorder. Diarrheas cause blood changes due to starvation, together with the effects of the parasites, poisons or other causes of the diarrheas. Chronic constipation without change in the intestinal flora causes little or no change in the blood picture. If purgative drugs are taken for the relief of the constipation some absorption of toxic materials may occur and this produces the changes characteristic of chronic intestinal toxemia. This condition produces the blood changes characteristic both of nutritive and of toxic anemia. The nutritive factors depend upon the diet of the patient. Intestinal toxemia is a form of poisoning which is often obscure and which causes a fairly characteristic blood picture. The symptoms are not definite; pallor, weakness, malaise, irregular periods of constipation and diarrhoea, bad breath, headache, visual disturbances, somnolence with restlessness most marked at night and some slowing of the reaction time are the most common manifestations of this form of poisoning. Blood pressure varies, pulse is usually slow, respiration irregular. The absorption of the products of putrefaction is the essential feature of the disease. Bony lesions which cause weakness of the musculature of the intestines, modify their circulation and cause related secretory abnormalities include the eighth thoracic to the second lumbar vertebrae. Rigidity of this part of the vertebral column is always present and a definite lesion is always shown by careful palpation or by stereoscopic X-ray plates carefully studied. The ultimate result of the lesion is an atonic area of considerable extent involving some part of the intestine according to the location of the lesion, with mild chronic congestion and disturbed secretory activity of the same area. The mucous secretion is increased through the affected area while the water and the enzymes are diminished. The alkalinity of the intestinal contents is increased. All these conditions tend to encourage the growth of putrefactive bacteria in the intestinal tract, and these bacteria break down the nitrogenous moiety of the food into substances poisonous to the human organism. The effects of these conditions on the blood cells are characteristic but not altogether pathognomonic. The red marrow of the lesioned vertebrae and ribs is affected and the cells produced in this area include many immature and reversionary forms. The poisonous substances absorbed act on all types of blood cells in some degree. (Plates III, IV) Small hyaline cells are always relatively and usually absolutely increased. When the lesion includes the ninth thoracic vertebra the increase is most marked. Atypical hyaline cells are present; these include cells which are larger or smaller than normal. Immature forms are variable and they seem to appear in the blood in showers. The lymphocyte nuclei are often lobed or indented and they may be double. Large hyaline cells are increased. Their nuclei are often lobed, indented, double or polymorphic. Large lymphocytes and endothelial cells are especially abundant. Plasma cells are rare or absent. Eosinophiles are usually increased slightly, both relatively and absolutely. If the abnormal intestinal content happens to include may protozoa or any of the vermes the eosinophilia may reach very high figures. Neutrophiles show serious changes. They are diminished relatively and usually absolutely. Immature and reversionary forms are occasionally present. Neutrophiles affected by the toxic substances show the changes characteristic of abnormal protein katabolism generally. The nuclei vary widely in their affinity for basic stains. The nuclear average is very high, often exceeding 3.50. Budding processes resembling nuclear pseudopodia and aberrant small masses of nuclear substance in the protoplasm are present. Nuclear forms are bizarre. The protoplasm in the immediate vicinity of the nucleus is often clear, free from granules, without any staining reactions. The granules have usually increased affinity
for eosin, though very often a few granules are definitely basophilic.
The intergranular hyaline protoplasm is rather more abundant and
more definitely basophilic than normal. The cell outlines are indefinite
and often ragged or frayed in appearance. Fragmented forms are abundant.
It will be noted that the findings just described resemble those present in carcinoma. This is to be expected since the poisonous factors are much alike. The changes are usually less pronounced in intestinal toxemia. The blood of the person with intestinal toxemia whose diet includes considerable amounts of meat and highly nuclear foods, such as sweet-breads, liver, kidneys and brains, shows cells which are very like those present in carcinoma. The alkalinity of the blood is usually increased in cancer, and is usually normal or low in intestinal toxemia. In intestinal toxemia an undifferentiated proteolytic enzyme may be present, but it is much less marked than in carcinoma, as a rule. In early carcinoma this enzyme may be present in a patient with high protein diet. In intestinal toxemia fibrinolysis may be normal; this has never been found true in carcinoma. Patients with intestinal toxemia may not have normal fibrinolysis. In intestinal toxemia the fibrin formation is considerably delayed in most cases and is scanty in amount; in cancer the fibrin threads are speedily and abundantly formed. In both intestinal toxemia and in cancer the refractile bodies may be increase; beaded, radiate and net-like forms of fibrin threads may be present or may be abundant. It must be remembered that intestinal toxemia and carcinoma may be present in the same person at the same time. Either condition exaggerates the cell variations due to the other sources of toxemia, since both produce similar effects. In order to differentiate between the blood
cell changes due to intestinal toxemia and those due to cancer or
to some other form of abnormal protein katabolism, it is best to
have the patient under observation for several days. During this
time his diet must be chiefly cellulose foods, such as fruits and
vegetables, and the intestinal tract must be as thoroughly cleansed
as is practicable. Thus the absorption of toxic substances from
the intestinal tract is avoided. Within a few days thereafter the
blood cells show decided tendency to normal structures if the toxemia
is of intestinal origin. Very great loss of blood is possible. Osler reported a patient with hematemesis who lost ten pounds of blood during one week, and who recovered from the effects of the hemorrhages. Ehrlich reported a case in which twenty kilograms of blood were lost during six and one-half months, with later recovery from the hemorrhages. Blood taken immediately after severe hemorrhage
shows little or no change. Within a few minutes the depleted blood
vessels take up liquid from the tissues and the blood shows the
low red cell count and hemoglobin count characteristic of simple
dilution. At first the color index remains unchanged, but within
a few hours increased numbers of immature or imperfect red blood
cells are thrown into the circulation from the red bone marrow,
and the low color index characteristic of secondary anemia is found.
Normoblasts appear in the peripheral blood within an hour or two
after the hemorrhage has occurred. Poikilocytes and microcytes appear
more quickly. These are frequently derived from red cells originally
of normal size and form, but distorted or fragmented as a result
of the plasma changes. Repeated losses of blood result in increased activity of the hematopoietic tissues. If the losses do not exceed the powers of these cells to replace the blood, no harm follows. The condition is that present during adult womanhood, during which time a loss of blood which may be quite considerable is replaced habitually, with no evidences of anemia. Professional donors of blood for transfusion show no evil effects from the losses. Even in cases of gastric ulcer, moderate hook-worm invasion, moderately severe cases of amebic dysentery and other hemorrhagic diseases there may be no recognizable anemia. But if the losses of blood are habitually beyond the regenerative ability of the bone marrow, anemia is inevitable. Anemia due to hemorrhages alone, before exhaustion of the bone marrow, is characterized by a red cell count reduced slightly or not at all; hemoglobin considerably reduced; leucocyte count usually above normal with a normal or almost normal differential count; increased activity of the neutrophiles on the warm slide with markedly increased activity of the eosinophiles; scanty fibrin threads slowly formed on the warm slide; subnormal viscidity of the blood; the formation of a very soft clot within normal coagulation time and, after the condition has been present for some months, the presence of normoblasts and myelocytoid leucocytes in the circulating blood. If the excessive loss of blood persists until
the hematopoietic tissues become exhausted the blood shows the characteristics
of aplastic anemia. No normoblasts or myelocytoid cells are present
in the blood and the lymphocytes alone remain normal in character
and in actual counts. The lymphoid tissues do not become exhausted
as a result of hemorrhage no matter how severe or how frequent the
loss of blood may be. Mrs. Q., patient in the clinic of The Pacific College of Osteopathy. Cervical polyp which extended into the vagina was the apparent cause of persistent uterine hemorrhage. Age of patient, 33 years. History included no factors of interest except that the polyp and hemorrhage had been present for about seventeen months before examination. Hemoglobin 12%; 16 grams per liter. One year, three years and five years later she
returned to report her condition. No abnormal conditions had occurred
during these years, except that she suffered a broken ankle once,
and several times contracted ordinary slight colds which yielded
at once to osteopathic treatment. The blood remained normal during
these years. Probably all secondary anemias for which really adequate cause is not found have a developmental anomaly of the hematopoietic tissues. Well-made people become anemic only under extremely severe conditions. The serious forms of developmental anemia are included with the primary anemias. The actual etiological agency in the developmental anemias lies in some abnormal conditions affecting the life of the patient during embryological or fetal existence, or the germ cells from which the embryo was developed. Heredity is sometimes the important factor. The germ cells, originally normal, may have been affected by some systemic disease of the parent. The embryo or fetus is, of course, subject to many abnormal conditions affecting intrauterine life. The most rapid development of the blood-forming tissues and the most rapid development of the central nervous system occur at about the same embryological period. This fact explains why persons with neuroses and psychoses associated with developmental imperfections of the nervous system usually show also some developmental anemia. The most marked form of developmental anemia is found in the rare congenital aplastic anemia. In this form the hematopoietic tissues, congenitally inefficient, fail to react to even slight demands. At autopsy the bones show only scanty and very pale areas of red bone marrow. The blood is watery, scarcely tinted; both red cells and hemoglobin are very low and the total leucocyte count is below 1,000 with 90% to 99% lymphocytes. Mild forms of developmental anemia are always found in persons who show other stigmata of degeneracy. The red blood cells and the hemoglobin are both diminished; the hemoglobin shows the most marked reduction. The red cells are small than normal, show considerable variation in size and in form and are more frequently basophilic than in normal blood. Nucleoids or other nuclear remnants are common. Normoblasts and microblasts are found in small numbers. The white cells are usually normal in number but include a high proportion of hyaline cells while the granular cells include many immature or atavistic forms. Amphophilic micromyelocytes are common. Atypical granules are frequently found in the protoplasm of hyaline cells and neutrophilic granular cells. Fibrin threads are scanty and of slow development. The clot is formed within a normal time but it is soft and does not retract normally. Platelets are usually below normal in number and they fail to agglutinate properly. These persons are often bleeders, and usually they suffer also from achlordhydria. (Plates V, VI, VIII) The achlorhydria might be expected to increase the severity of the anemia, though in ordinary cases these patients, with mild developmental anemia with achlorhydria or hypochlorhydria do not display any lower hemoglobin than do those with normal hydrochloric acid in the gastric juice. On the other hand, the lack of hydrochloric acid in the gastric juice of patients with typical pernicious anemia must be considered in this connection. The prevention of developmental anemia in the next generation should be reasonably easy. If the youthful members of this generation receive adequate osteopathic treatment, and if they live reasonably hygienic and sensible lives, there should be few or none of these cases among their children, and probably none among their grandchildren. Even now it is difficult to find cases of this kind in the children of families accustomed to osteopathic attention. The treatment of the developmental anemias is
necessarily rather unsatisfactory to those wishing complete restoration
to normal conditions. Very pleasing results are, however, sometimes
secured. It is possible only to provide the imperfectly developed
hematopoietic tissues with the conditions best adapted to their
conditions. Structural relations as nearly normal as is practicable,
excellent hygienic conditions and the avoidance of all excessive
demands upon the blood forming tissues often lead to the development
of blood which is good enough for all practical purposes and thus
to symptomatic recovery from the anemia. These unfortunate individuals
must always avoid infections, fatigue, malnutrition and any cause
of toxemia with much more than ordinary care. Nearly all forms of secondary anemia are associated with at least some toxemia. There are many drugs used in the treatment of disease which ultimately cause anemia. Diseases of several different viscera are associated with marked anemia and toxemia. The poisons associated with fatigue, the absorption of degenerating proteins of the body itself or of exogenous materials all cause anemia, if the process is long continued These varying conditions produce varying changes in the blood cells. The history of the patient with reference to the use of drugs is usually sufficient for diagnosis, if the facts can be discovered. The habitual user of drugs is often unaware of the serious nature of his addiction. A patient in the clinical laboratory of The A. T. Still Research Institute suffered from such a toxemia. He denied using drugs except some small homeopathic doses once in a long while, for cold or toothache. But persistent questioning of the patient and, finally, of his wife, disclosed the fact that self-drugging had, in his case, reached an extreme of habitual poisoning. The effects produced vary with the character of the drugs which are used. Habitual use of purgative drugs causes changes in the blood characteristic of chronic starvation. The use of thyroid extracts causes increase in the mast cells in the circulating blood. Nearly all of the coal tar derivatives and the salicylates cause a mild but persistent hemolysis with the blood changes of typical secondary anemia. Camphor and irritating fumes cause eosinophilia together with the usual characteristics of secondary anemia if the use of the drug is persistent. Chronic lead poisoning causes secondary anemia which is often confused with pernicious anemia. The color index is near unity. Megalocytes, megaloblasts, basophilic stippling, low leucocyte count, high nuclear average, all are frequently found in chronic lead poisoning and may cause confusion in diagnosis if the history of the patient does not explain the findings. (Plate VII) Lead poisoning causes loss of normal elasticity
of the red cells with increased fragility on the warm slide. The
cells are more resistant to changes in the osmotic tension of diluting
fluids than are normal cells; this is probably due to the fact that
the lead seems to affect only the periphery of the erythrocytes.
The blood is less viscid than normal and the cells lose their normal
stickiness. The Rouleaux are extremely scanty, and in many cases
none are formed in an ordinary warm-slide preparation. Fatigue toxins cause fairly constant changes in the blood cells. In chronic fatigue the usual indications of secondary anemia are present in the blood cells, together with indications of toxemia of a peculiar type. The red cells are softer and more fragile than normal. On the warm slide they are easily distorted by the pressure exerted by other cells carried along in the currents of plasma, and after such distinction they do not regain their original form for some seconds after the pressure is released if the currents are rapid the cells frequently become fragmented, forming two to several very small masses which become rounded within a few seconds. These cells resemble microcytes, and in many instances cannot be distinguished from the microcytes found in the dried smears of blood. The hyaline cells vary in size, and include a few which are larger and a few which are smaller than those found in normal blood. Atypical granules are often found in these cells. Neutrophile nuclei are swollen and have ragged or frayed outlines, but pseudopod-like processes and aberrant nuclear masses are absent or rare. The neutrophilic granules include many which are larger than normal. Eosinophiles frequently show three or four nuclei, and these often present ragged or frayed outlines. Mast cells are increased slightly. Myelocytoid forms are present, though rarely in any considerable numbers. Differential staining is more difficult than in normal blood. In severe fatigue many masses of pale nuclear material without any recognizable cytoplasm may be found lying free in the plasma. Occasionally a few granules in the immediate vicinity of such nuclear masses indicate the type of cell which has been destroyed. More often there is no identifying structure. These nuclear masses become thinner and more irregular in outline, then less definitely basophilic, and finally seem to dissolve completely. Fibrin threads are scanty and are formed after ten to twenty minutes. Refractile particles are abundant; these include sudanophilic and iodophilic granules. Rouleaux are formed slowly and are often imperfect. This blood picture is sufficiently distinct to differentiate fatigue from certain definite diseases. When fatigue complicates some chronic disease the blood findings may be puzzling or even misleading. For this reason the patient with a chronic disorder who is weary should be allowed to rest for an adequate time before the blood is taken for examination. In acute diseases the effects of the fatigue toxins are usually masked by the effects of the acute disease. Treatment of secondary anemia due to fatigue is difficult. There is very often a developmental basis for the anemia because normal people do not exert themselves to such an extent, except under extremely severe and unusual environmental circumstances. Normal people react to even serious fatigue and anemia is absent or temporary. Neurotic persons find rest difficult, especially after fatigue becomes profound. Persons with developmental anemia are often neurotic and often lack the self-control essential to rational alternations of work and rest. For these reasons treatment is difficult. In order to secure recovery the treatment for
ordinary forms of secondary anemia must be modified. Complete rest
is sometimes best; in other cases a moderate activity is essential
to good nutrition and good circulation of the blood through the
red bone marrow. Various methods of elimination of the toxins may
be helpful; these include adequate drinking of water, fruit juices
or milk, according to the general condition of the patient; hydrotherapy
is occasionally useful. The most important factor in these cases,
as in other forms of secondary anemia, is the maintenance of a good
circulation of the blood through the ribs and other fields of hematopoiesis.
The products of putrefaction or degeneration affect the blood cells seriously. Malignant neoplasms, degenerating pyogenic foci, degenerating cystic masses, degenerating benign tumors, resolution and absorption of the products of abnormal protein disintegration cause the blood cells to show certain traits which are quite characteristic. Chronic intestinal toxemia has already been described. The red cells may be affected slightly or seriously, according to the nature of the toxic substances. Many of these are definitely hemolytic, such as the products of certain malignancies, the poisonous substances produced by the activities of the hemolytic streptococci and the substances absorbed from the intestinal tract containing an excess of putrefactive bacteria acting on a diet rich in purins. In these cases the red cells are very pale, include a large number of Poikilocytes and the count may be low or normal. The hemoglobin is always low. The hyaline cells are usually normal in structure and are normal or only slightly increased in numbers. The eosinophiles are somewhat increased and they include many myelocytoid forms. The neutrophiles show nuclei which stain deeply, have definite and sharp outlines and which show peculiar processes which resemble the pseudopodia of the protoplasm of active cells. Very small masses of nuclear material lie in the cytoplasm, often near the periphery of the cell. The entire nucleus is occasionally very eccentric. The nuclear average is high, often reaching 3.5 or more. Fibrin threads are abundant and are formed speedily.
They are often irregular in outline and may be definitely beaded.
They seem to radiate from groups of platelets. Often the fibrin
threads are rather flattened and form an irregular mesh-like structure
on the warm slide. Refractile granules are more abundant than normal;
they rarely include any sudanophilic or many iodophilic granules;
unstained granules are very abundant. Cases characterized by abnormal increase in the red blood cells are much less common than are the anemias, but they do occasionally occur. The simplest form of polycythemia occurs as a reaction to some abnormal environmental condition, or is produced by some abnormal abstraction of water from the blood. Erythrocytosis is an abnormal increase in the number of red cells per cubic millimeter of blood, due to some physiological or pathogenic condition. Premature infants show polycythemia during the first few days of life, as do normally born babies. Physiological Erythrocytosis occurs in mild degree during the early afternoon and the early morning hours, usually about two oclock in each case. At this time the red cells may be s much as 1,000,000 per cubic millimeter above the counts taken at about eight oclock but usually the variation is less than 500,000 cells. The hemoglobin varies with the varying red cell count, so that the color index remains practically unaffected. In making successive counts for the same patient and in comparing counts made for different patients it is necessary to make due allowances for this source of variation. In our laboratories it is a custom to make as many of the counts at about two oclock as is practicable, and when this cannot be done we made successive counts for the same patient at the same time of day. This early afternoon erythrocytosis was attributed to the changes due to the digestion of food, in earlier days, but it has been found that the rise occurs whether the patient has eaten or not. Persons who do not eat during the day at all, persons on a long fast, and persons who eat ordinarily heavy meals at noon, habitually, all show about the same Erythrocytosis during the early afternoon hours. Only when some person who has been fasting or has been eating very abstemiously eats a meal heavy in proteins is there a recognizable digestion Erythrocytosis; this condition goes with the digestion leucocytosis in extent and, very probably, in cause. Persons who ascend to high altitudes rather suddenly may show an increase in red cells sufficiently marked to be called erythrocytosis. In many such cases the blood cells include immature forms, and normoblasts may be abundant. Erythroblasts and megaloblasts are occasionally found, and this condition should be classed as pathological rather than physiological. Many abnormal conditions may cause erythrocytoses just as certain abnormal conditions may cause leucytoses. Heart disease causes erythrocytosis which may be extreme; in an osteopathic clinic a child with congenital mitral lesion had a red cell count of 8,500,000 cells. Other cases with counts of 9,0-00,000 cells have been reported for congenital heart cases. Disease of the mitral valve causes more constant and more marked erythrocytosis than do diseases of other valves. Adherent pericardium and chronic pericarditis without adhesions also cause erythrocytosis. Functional cardiac disorders cause less marked increase in the red cell count; rarely the count exceeds 6,500,000 in our records. The total blood volume remains unchanged. The functional cardiac inefficiency due to lesions of the fourth thoracic vertebra (less commonly the third or the fifth thoracic vertebra) causes an increase in the red cell count, rarely to more than 6,500,000. Cardiac weakness due to malnutrition or to toxemia also may increase the red cell count; in these conditions the hemoglobin is usually quite low and the color index may be 0.5 or less. Lowered oxygen tension in the tissues is one factor causing this erythrocytosis. Chronic pulmonary diseases may cause puzzling increase in the red cell count. Especially those diseases characterized by severe attacks of coughing often show high red cell count, and these cells may present a remarkably normal appearance. The act of coughing causes increased circulation through the red bone marrow of the ribs and no doubt this is one factor in the erythrocytosis present in certain cases of tuberculosis, chronic bronchitis and other pulmonary diseases. Diminished oxygen tension in the hematopoietic tissues leads to increased development of red cells. Septic cases usually show some erythrocytosis
during the acute stages. Pneumonia also shows erythrocytosis during
the early days, and this may persist through the course of the disease
and for some weeks after recovery. No doubt the stimulus to increased
leucocytogenesis caused by pyogenic infections affects the erythrocytogenic
areas of the bone marrow also. In chronic pyogenic infections, anemia
and leucopenia are often present; this is due to exhaustion of the
hematopoietic tissues. Occasionally this exhaustion terminates in
anemia resembling the pernicious form; more often the terminal anemia
is of the aplastic type. Vomiting, diarrhea, excessive sweating and other conditions which abstract water from the blood cause mild increase in the red cells which rarely rises to a degree warranting the term of erythrocytosis. The blood quickly takes up water form the tissues to replace the loss, except in cases of profound desiccation, and the erythrocytic rise is usually transitory. Profound desiccation such as follows long exposure to severe and very dry heat may cause erythrocytosis to 7,000,000 or more; this occurs in persons lost in the desert or in high mountains. Erroneous diagnosis of erythrocytosis may be
made if the technique of taking the blood is not accurate. If the
area to be pricked is handled too much or is washed with any irritating
substance so that the capillaries are dilated, the red cell count
may be increased by as much as 2,000,000 cells per cubic millimeter.
If the correct count is 5,000,000 or more, such an error in technique
might easily lead to mistaken diagnosis of erythrocytosis or erythremia.
This is a disease for which no adequate etiology is known. No definite bony lesions have been found with apparent etiological significance. It is characterized by abnormally increased formation of red cells, just as leukemia is characterized by abnormally increased formation of white cells. The spleen is always somewhat enlarged and it may be as large in erythremia as in lymphatic leukemia, though it rarely approaches the enormous size occasionally found in splenomedullary leukemia. A lesion of the ninth thoracic vertebra is occasionally present, and the correction of this exercises a temporary effect upon the size of the spleen, but in many cases no such lesion is found, and the effect produced by its correction is never permanent. The disease usually appears during middle life or early old age. The symptoms are not pathognomonic. Cyanosis is the most common symptom and this may be severe; an incorrect diagnosis of cardiac or pulmonary disease is easily made if the blood is not examined. The mucous membranes and the skin may show a peculiar brilliant cherry-like tint. In one of our cases there was an old bronze-like pallor which suggested disease of the adrenals. The systolic and the diastolic blood pressure may both be considerably increased, and the pulse pressure is usually slightly below normal. Gross or petechial hemorrhages of the mucous membranes are fairly common and the cyanosis is relieved when these occur. Therapeutic bleeding diminishes the symptoms temporarily and diminishes the danger of excessive spontaneous hemorrhages. Apoplexy frequently occurs and is a common cause of death. Increased pressure of the cerebro-spinal fluid is a common condition in erythremia and this causes various symptoms of vertigo, tinnitus, headache and peculiar disturbances in the sense of time, personality and space-relations. These symptoms are all temporarily relieved by removal of a very few cubic centimeters of spinal fluid, and are usually relieved by the occurrence of a spontaneous hemorrhage or by therapeutic bleeding. The blood picture is characteristic. In three
cases examined in our laboratories the counts were 7,400,000, 7,700,700
and 8,200,000. Counts of 13,000,000 and more have been reported
by Osler and others. Counts below 7,000,000 should not be included
unless other findings are pathognomonic. The color index does not
fall much below one, and is almost never above one. The hemoglobin
varies from 120% to 150%, and in our cases was 150%, 135% and 130%,
Dare. The increased activity of the hematopoietic tissues is usually but not always limited to the red cells. Associated leucocytosis is rare, and is always limited to the granular cells and myelocytes. Even when no leucocytosis is present a few myelocytes can be found on careful search. McAlpin reported a case of polycythemia rubra with a red cell count of 9,400,000 and hemoglobin of 128% in which the white cells rose to 96,000 before death. The spleen was extremely large in this case The leukemia was of the spleno-medullary type. Lymphocytes remain normal in actual numbers, though the percentages vary with the varying counts of granular cells. Leucopenia occasionally occurs; this also is
due only to diminished numbers of the granular cells. The actual
number of the lymphocytes remains constant. No treatment gives permanent relief. Bleeding relieves the symptoms but the effect is transitory. X-ray treatment of the skeleton diminishes the speed of red cell formation for a few weeks. Correction of lesions affecting the spleen give temporary relief, if such lesions are found on examination. The course of the disease is like that of chronic lymphatic leukemia. Death occurs from apoplexy, hemorrhage, heart failure or some intercurrent disease. |
{kind=link}