
| Primary anemias are those forms of anemia for which no adequate cause is known. With increasing knowledge of the relations between structural abnormalities, hygienic improprieties and the formation of the blood cells, the cases called primary or idiopathic are slowly diminishing in numbers. Pernicious anemia, chlorosis and aplastic anemia are the most common of the primary anemias. Simple primary anemia is already known to be a misnomer. This is by definition a form of anemia without known adequate cause, which progresses through many remissions, with no intermissions, until death occurs from asthenia or from some relatively mild intercurrent disease. The cell count in these cases is rather high, the hemoglobin low, the leucocyte count almost or quite normal with relative excess of the small hyaline cells. This form of anemia is due to malnutrition and to rib lesions, and is, therefore, really a form of secondary anemia. It is evident that no abnormal condition can occur without adequate cause. In the primary anemias there is some congenital defect. Very often individuals with such defects are able to live normal lives so long as no excessive demand is made upon the hematopoietic tissues, provided always that environmental factors remain good. When these persons fail to receive the best of food, adequate rest, sufficient sunshine or fresh air, or when any infection or other cause of disease occurs, the defective hematopoietic tissues are speedily overcome by the increased burdens. Fatal or very serious anemias supervene unless the etiological factors are speedily recognized and removed. The causes of the developmental defect have not been well studied but are probably identical with the causes of many other aberrancies of embryological life. Experiments made upon animals in many laboratories have shown that embryological development can be easily modified. The breathing of fumes of alcohol, ether, chloroform, mercury, illuminating gas and any other abnormal volatile substance by either male or female guinea pigs, rats and other laboratory animals causes the appearance of many deformed young in the progeny. Exposure of incubating eggs to such fumes and in excess of carbon dioxide increases the number of deformed chicks, sometimes to 90% or more. Addition of abnormal substances to the water containing gametes of any living creatures increases the number of deformed ova or embryos. Both male and female germinal cells are affected by such poisons. Drugs administered to either males or females before
mating increases the number of deformed young, and this applies to mammals
and to submammalian genera.
Human embryos found at operations for tubal pregnancy include a larger proportion of deformities than are found in uterine pregnancies; this is undoubtedly due to the abnormal environment of the developing embryo. In the laboratories of The A. T. Still Research Institute the progeny of animals with bony lesions always show some developmental defects. From all these findings it may be concluded that
developmental defects may be due to some abnormal condition affecting either
the sperm cell or the ovum cell before union; abnormal conditions affecting
the ovum after fertilization and before its fixation in the uterus, and
abnormal conditions affecting the embryo and fetus as a result of maternal
disease or poisoning.
Aplastic anemia is a rather rare condition characterized by aplasia of the red bone marrow. The cause is not known, but the nature of the findings on blood examinations and autopsies strongly indicates a developmental basis for the disease. In adult life a similar condition occurs, apparently as a result of exhaustion of blood-forming tissues which are unable to meet some excessive demand. Osteosclerotic anemia is a very rare disease in which there is an increasing growth of bone or of dense fibrous tissue into the red bone marrow. The anemia is of the aplastic type after the disease has become well established. Albers-Schonberg disease is a form of osteoscleroic anemia occurring in childhood. The bones become hard, solid and brittle and fracture easily or spontaneously. The red marrow is invaded by bone or fibrous tissue and the anemia is of the aplastic type. Differential diagnosis between these various anemias of the aplastic type is difficult. Biopsy of a fragment of rib may determine the true nature of the disease. True aplastic anemia occurs in young people and children, usually after some disease which has affected the blood. The disease is characterized by marked anemia with no evidences of regenerative activities on the part of either leucocytopoietic or erythrocytopoietic tissues, and by a rapid progress to an inevitably fatal ending. Hemorrhages are frequent. The skin and the fat of the body are very pale. At autopsy the red bone marrow is scanty and may seem to be completely absent, the cavity of the bone being occupied by dry connective tissue fibrillae within whose meshes a few small, pale, dry areas of atrophic bone marrow may occasionally be found. The differential diagnosis between anemia and aplastic anemia may be indicated by the following comparison: Pernicious anemia Aplastic
anemia
The following case is not quite typical because the color index was very variable and occasionally high and because nucleated red cells were found in the blood before death. E. E. A young man eighteen years old, never robust but always well until he was sixteen years old, when he suffered a rather mild attack of malaria. Thereafter he became progressively weaker and more emaciated. At the first examination the blood count was as follows: Hemoglobin 26% (33.6 gms. per liter, vonFleischels apparatus) Red cells 2,320,000 per cu.mm. (46%)
Hemoglobin 25% (33.2 grams per liter, von Fleischls
apparatus)
The treatments were useful in that the patient seemed
stronger, suffered less dyspnea and showed some color in the skin. The
course of the disease was not
Hemoglobin 15 grams per liter (10.5%)
Hemoglobin 24.8 grams per liter (18%)
(Progressive pernicious anemia; hemolytic anemia; Addisonian anemia; cryptogenic anemia; primary progressive anemia. Pernicious anemia is a disease of unknown origin,
characterized by its chronic and intermittent progressive weakness to death;
hypertrophy of the red bone marrow, and blood showing low hemoglobin, high
color index and the presence of megaloblasts and other immature blood cell
forms.
Many factors have been discussed as probable causes of pernicious anemia. That there is some adequate cause of every abnormal condition is axiomatic, but for this, as for several other very serious diseases, no such cause has yet been found. Infection by hemolytic bacteria; the presence of hemolytic products of abnormal katabolism; proliferative activity of the bone marrow resembling the proliferative activities of malignant neoplasms; the lack of some food material necessary to the manufacture of normal red cells, and the presence of some developmental defect in the hematopoietic tissues have all been considered etiological factors. Perhaps several of these factors are essential to the development of the disease; perhaps some other condition, as yet unsuspected, will be found the essential cause of pernicious anemia. The occurrence of intermissions, during which the health of the patient and his blood picture seem perfect, is one of the most puzzling features of this disease. In one of our cases the last remission lasted for eleven years, after which relapse was extremely rapid and quickly fatal. Even longer intermissions have been reported. The blood cells include many embryonic and occasionally atavistic cells; the color index is always high, usually exceeding unity, and leucopenia is always present in typical cases. Forms of secondary anemia resembling pernicious anemia are found in patients suffering from bothriocephalus latus; in this case a lipoid substance extracted from the worm is distinctly hemolytic. Infection by streptococcus hemolyticus sometimes causes a blood picture of the pernicious type. When cancer metastases invade bone marrow the blood may resemble that found in pernicious anemia. There are several less common conditions in which the diagnosis between pernicious and extremely severe and atypical secondary anemia is very difficult. In one of our cases a balantidium coli infection caused blood findings typical of pernicious anemia. Sprue and other tropical diseases may also cause a blood picture like that of pernicious anemia. True pernicious anemia may begin during pregnancy. In many cases a form of anemia resembling pernicious begins during pregnancy, and this is associated with a mild leucocytosis. It disappears soon after labor. In other cases the anemia may not seem to be more severe but it does not disappear after the termination of pregnancy. In one of our cases an anemia with hemoglobin of 45%, color index of 1.2 and typical megaloblastosis was found at the fifth month of pregnancy. Within three weeks after the birth of the child the hemoglobin had reached 85%, with a color index of 0.7. Pernicious anemia rarely occurs in children, and in the few cases reported achlorhydria has also been present, as is the case with pernicious anemia in adults. Children kept too long on milk, especially on goats milk, may develop an anemia which resembles the pernicious form very closely. In this case the hydrochloric acid of the gastric juice is normal, and recovery follows the establishment of a normal diet, though sometimes convalescence is prolonged and stormy. Typical cases of pernicious anemia have been reported in wild mammals kept in captivity, by Fox and others. The symptoms can be given only briefly in this discussion. The patient is rarely emaciated; the skin presents a typical lemon-yellow tint; achlorhydria is always present in typical cases and indigestion due to this factor is almost always noted; gastric pain and persistent diarrhea are common. Glossitis, often with ulceration, and pyorrhea alveolaris are usually present. Weakness, palpitation, headache, dyspnea, vertigo, edema of the extremities and the face, neuritis and various forms of tingling, numbness and other nervous phenomena are very common. Late in the disease degeneration of different areas of the central nervous system causes symptoms which may or may not be related to the site of recognizable degenerative processes. Degenerative areas of considerable extent may occur without causing symptoms; this is true also of other degenerations within the central nervous system. The course of the disease varies greatly. Sometimes
death occurs within a few weeks after the first symptoms are noted. More
commonly, several periods of intermission or remission occur before the
terminal attack; very often death occurs from some intercurrent disease.
Diagnosis is usually easily made from the blood picture. In one of our cases, and in many reported cases, the nervous symptoms have been misleading and blood examinations postponed until the pallor or the characteristic skin tint led to further investigation. In atypical cases the diagnosis may present great difficulty. In selected cases it may be advisable to remove a bit of a rib for a study of its marrow, in order to determine the essential nature of the disease. Chemical examination of the blood has not given useful information. The specific gravity is low, often below 1,027. The osmotic tension remains normal or increased. The high osmotic tension with low specific gravity is due to the fact that iron and the large organic compounds are diminished while the smaller inorganic molecules are increased. The blood sugar may be increased or may remain unchanged. The nitrogenous wastes are increased, as is inevitable with nephritis due to the anemia. The alkaline reserve is frequently diminished. According to Rowntree, the total blood volume in pernicious anemia is lower than normal, hypovolemia. Of nine cases only one showed normovolemia. The average was 76.4 cubic centimeters of whole blood and 58.8 cubic centimeters of plasma per kilogram of body weight. The blood serum is deeply pigmented, but there is no marked excess of bile pigments. The urine is paler than normal in most cases. Platelets are greatly diminished and it may be impossible
to find any. The coagulability of the blood is decreased, and there may
be no clot formed at all. The viscidity is very low and the blood seems
to be as thin as water. The water of the blood is greatly increased and
may exceed 90% of the weight. The albumin of the blood plasma is not modified,
though the albumin of the cells is greatly diminished. In this respect
the blood in pernicious anemia differs from the blood in equally severe
secondary anemias. The cholesterin is greatly diminished and the fats of
the blood substantially increased. Fatty globules are frequently found
in the blood smears, both within the neutrophiles and lying free in the
plasma.
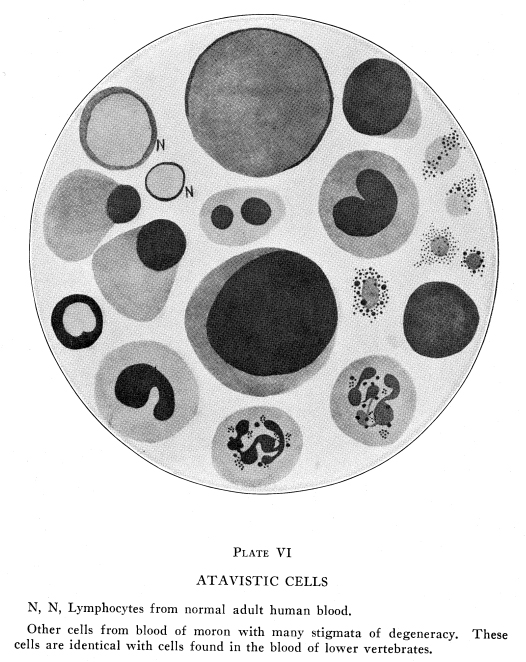
PLATE VI
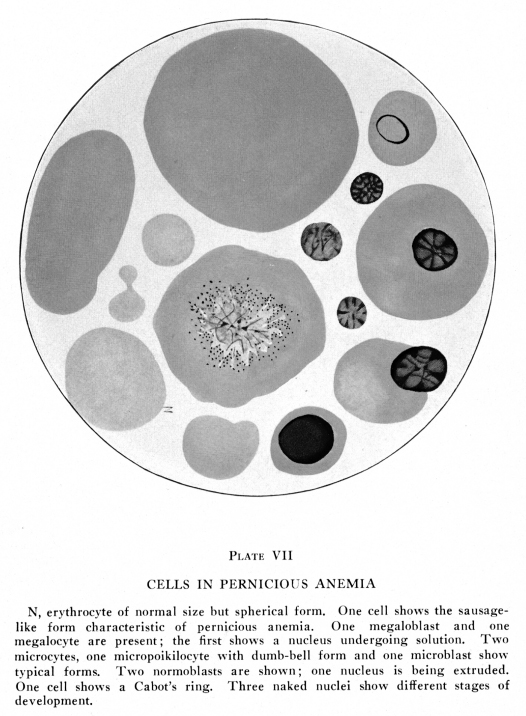
The red cells show characteristic changes, though
these are not absolutely pathognomonic. Hemoglobin may be diminished to
10% of the normal for the age of the patient. Red cells are diminished
more than the hemoglobin, and the color index is always high in typical
cases without recent transfusion. Nucleated red cells of many types are
present. Cells showing various endoglobular structures, nuclear remnants
and basophilic stippling or reticulation are abundant. Poikilocytosis is
less marked than anisocytosis and the Megaloblasts more numerous than Normoblasts
in typical active cases. Edematous cells are frequently found. (Plate VII.)
The red cell count may be very low, and is usually about 2,500,000 at the first examination, in our cases. Counts as low as 500,000 are found and patients with these low counts may be comfortable and reasonably active. The hemoglobin may be as high as 18% with a red cell count of 9% of the normal for the age and sex of the patient. The volume index is always above one in typical cases, but the amount of hemoglobin carried by a given volume of erythrocyte protoplasm is less than normal; the saturation index is low. Anisocytosis is more marked in pernicious anemia than in any other disease. Microcytes (from 2 microns to 6 microns in diameter) are abundant. They may be very dark in color; this is due to their spherical form. Macrocytes and megalocytes (9 microns to 16 microns in diameter) are abundant. They may be spherical and appear very dark in color, or they may be flattened and seem to be very pale. Gigantocytes exceed l6 microns and may reach 20 microns or more in diameter. They often appear during the last few days of life. Both microcytes and the very large cells often show a tinge different from that found in normal cells, as if some abnormal pigment might be associated with the hemoglobin. Poikilocytosis is less marked than anisocytosis but is abundantly present. Sausage-like forms are especially abundant, though all the ordinary types of Poikilocytes may be found. Polychromasia is abundant. Basophilic reticulation and stippling occur in young cells. Degenerative forms may also be basophilic. They are most abundant in the severe cases. Megaloblasts, gigantoblasts and megakaryocytes are found in the blood in order according to the severity of the case. In typical cases Megaloblasts exceed Normoblasts. Erythroblasts are usually more common than Megaloblasts in mild cases. Megakaryocytes and gigantoblasts usually appear only in very severe cases approaching death. Microblasts, poikiloblasts and Normoblasts vary considerably in the same patient at different times; their numbers do not seem to bear any definite relation to the severity of the disease. Blood crises are fairly common occurrences. The bone marrow undergoes suddenly increased activity and a shower of blood cells is thrown into the circulation. These cells may be almost or quite normal and an intermission or a remission occur. The cells may include great numbers of nucleated and immature cells, in which case a more rapid progress of the disease is to be anticipated. If normoblasts exceed megaloblasts the prognosis is better than when great numbers of the very large nucleated forms are present at the time of a crisis. The more abundant the large nucleated cells, the more gloomy is the prognosis. The leucocytes are always diminished in typical cases, and a high leucocyte count should lead to very careful search for some definite etiological factor. A diagnosis of pernicious anemia is not warranted when leucocytosis is present until some complicating infection or other leucocytogenic factor has been found. The leucopenia has reached 3,000 cells in many of our cases, and has reached 1,000 several times. Counts as high as 6,000 occasionally occur in otherwise typical cases. The leucopenia is due to diminished neutrophiles count; the hyaline cells usually remain normal in actual numbers and in cell characteristics. With the changing count of granular cells, the hyaline cells show varying percentages, but their actual numbers remain almost or quite steadfast throughout the entire course of the disease. In those cases in which the blood is highly toxic, there may be mild absolute as well as relative lymphocytosis. In cases characterized by marked malnutrition, with wasting, the lymphoytes may be absolutely increased. The neutrophiles show nuclei of a peculiar rosette-like structure. These nuclear rosettes are not so abundant nor so perfect in any other disease The nuclear average is much higher than normal, reaching 3.8 in one of our cases, and usually exceeding 2.7 in typical cases. The eosinophiles are somewhat increased both relatively and absolutely. Moderate increase in eosinophiles is often associated with beginning remission. Sudden diminution in the eosinophiles is of grave significance. Mast cells are usually increased. myelocytes are always present and they may be abundant; these include neutrophilic, eosinophilic, basophilic and hyaline in the order mentioned. Extremely large myelocytes in the peripheral blood usually presage speedy death. With increasing hypertrophy of the erythrocytopoietic
tissues, the leucocytopoietic tissues may be variously affected. There
is usually atrophy of the latter, so that leucopenia increases steadily.
In other cases there may be some hypertrophy of the leucocytogenic areas
of the red bone marrow also. The white cells thus thrown into the circulation
include great numbers of myelocytes and the blood picture may resemble
that of leukemia.
The weight of the body remains constant or increases moderately, in typical cases. The fat is not diminished and there is a varying amount of edema of the tissues. Patients who lose steadily in weight should be subject to very careful examination in the hope that some adequate cause of the anemia can be found and removed. Degenerative processes affect the central nervous system after the disease has been present for some time, and this time varies greatly. It is not rare for the patient to seek relief for some nervous disorders before the anemia is suspected. In other cases no nerve degeneration appears at all, though the patient may die after several severe relapses. Nervous symptoms do not always bear a definite relation to the anatomical location of the degenerative processes. At autopsy areas of the nervous system may seem to be structurally normal after the symptoms have apparently indicated definite local degeneration, and, on the other hand, areas of marked degeneration may be found at autopsy although no symptoms referable to the affected areas were noted during life. The degenerated areas do not seem to follow any definite anatomical or physiological course. The constant lack of hydrochloric acid in the gastric juice of patients with pernicious anemia is of interest. The achylia precedes the anemia and persists during remissions without change. The very frequent lack of hydrochloric acid in patients with malignant neoplasms is of interest in this connection. The achlorhydria of pernicious anemia is not like the hypochlorhydria due to lesions of the sixth and seventh thoracic vertebrae, since in the latter cases the correction of the lesion results in a gradual return of the normal gastric secretion. In pernicious anemia and in the achlorhydria associated with malignant neoplasms of developmental origin, no treatment causes a return to normal gastric secretion. There is much reason for believing that this form of achlorhydria is due to some developmental defect whereby the oxyntic cells fail in proper differentiation. Persons showing other evidences of imperfect development, mentally or physically, very often suffer from achylia, achlorhydria or hypochlorhydria. PATHOLOGY
Autopsy findings are confusing. If death occurs during an intermission there may be nothing found anywhere to indicate pernicious anemia. The bone marrow may be of normal structure and normal location; the fatty marrow may occupy its normal position in the long bone. Liver and spleen may be normal in gross and in microscopic structure. If death is due to accident, the entire body may appear to be perfectly normal in every way. If death results from intercurrent disease, the autopsy finding may be only those of the fatal disease, with nothing to indicate pernicious anemia. More commonly death occurs from some other disease during relapse or remission, in which case variable indications of pernicious anemia may be found. In one of our cases death occurred from pneumonia, and the autopsy findings included those of pneumonia as well as those of pernicious anemia. In this case the anemia had just begun to grow more severe, after a remission of moderate degree lasting several months. When death occurs during the progress of the disease the autopsy findings are distinctive and easily recognizable, but they do not explain the nature or the cause of the disease. Although the blood is so deficient in iron, this metal is stored abundantly in the liver, both in the Kupflex cells and in the hepatic cells; the reticulo-endothelial cells of the bone marrow and of the spleen also contain iron more abundantly than normal. The red bone marrow shows marked hyperplasia and extends into the areas normally occupied by the yellow marrow, which it may completely replace. The solid parts of the bones may be so seriously invaded that they break spontaneously; this is especially true of the ribs. Areas resembling the erythrocytopoietic tissues of the embryo may be found in the spleen, liver and other glandular and lymphoid tissues of the body. Careful examination usually shows these cell groups to be composed of masses of endothelial cells, some of which are ingesting the abnormal red cells. They are, therefore, destructive and not constructive so far as the red cells are concerned. Phagocytosis of the red cells by the endothelial
cells is much more abundant in post-mortem than in biopsy material. This
indicates that at least part of the phagocytosis is a terminal or a post-mortem
phenomenon. The moderate degree of fatty degeneration, the moderate desquamation
of the Kupffer cells, their moderate hypertrophy and their phagocytic activities
in pernicious anemia do not seem greatly different from similar conditions
found in severe infectious or toxic diseases. Hence these phagocytic activities
do not seem to be the most important factor in pathogenesis The fat of
the body is deep yellow, sometimes definitely orange in color. The blood
may be so pale as not to be recognizable as blood when removed from the
vessels. All the organs are extremely pale and they may seem almost completely
bloodless. Areas of degeneration may be found within the central nervous
system, even in cases in which no nervous symptoms are presented before
death. Other organs show degenerations due to the long-continued anemia
and toxemias. The blood volume is not greatly modified, and the apparent
bloodlessness of the tissues is due to the pallor of the blood.
Methods of treating pernicious anemia have changed frequently with changing views of the etiology and the pathogenesis of the disease. Since no definite structural lesions have been found responsible for the disease, there is no specific osteopathic treatment for it. Patients with pernicious anemia are as subject to the evil effects of lesions as are other persons, and such lesions as are found on examination should be corrected. Very often such corrections are followed by marked relief of the symptoms. In this, as in almost all other diseases, it is the actual condition of the patient and not the name of the disease which determines the most efficient therapeutic methods. Since the hydrochloric acid deficiency is of developmental origin, little can be done to correct the condition; it is probably impossible to further developmental progress in persons old enough to suffer from typical pernicious anemia. Attempts have been made to provide artificial gastric juice for these patients. Occasionally the administration of hydrochloric acid, with or without pepsin, has been followed by marked and prolonged remission or intermission. In a patient for whom we made many blood examinations, the administration of an artificial gastric juice was associated with an intermission of eighteen years. At the end of that time the anemia suddenly became worse and he died within a few weeks. Splenectomy was at one time a favorite method of treating pernicious anemia. This was because an abnormal spleen was supposed to destroy the fragile red cells too rapidly. After splenectomy the red cells become more resistant and the anemia often diminishes for a time. The progress of the disease is only temporarily delayed at best, and no good results are visible at all, in many cases. Toxemia is always present in patients with pernicious anemia, and any rational methods of therapy must include careful attention to this phase of the disease. The administration of liver and of certain other nitrogenous foods containing considerable amounts of nucleins causes speedy intermissions with return of the blood to almost or quite the normal picture, in many cases. If patients die from some intercurrent disease during such an intermission, there may be slight or no indications that the patient had ever suffered from pernicious anemia. The intermissions may be prolonged almost indefinitely by persistent careful feeding. Yet, on relatively slight carelessness, the pernicious anemia blood picture may supervene with extreme rapidity and the patient may die within a few weeks from pernicious anemia despite the most careful feeding and care. The rapid improvement in the blood picture and in the general condition of the patient as a result of feeding these particular foods may lead to the inference that pernicious anemia is really a deficiency disease. A pre-existing cause of severe toxemia is almost always present in pernicious anemia, and while these conditions do not cause pernicious anemia except in certain people, yet there is much evidence that the toxic products of pyogenic foci and of intestinal putrefaction have some etiological relation to the disease. The fact that some developmental defect is necessary for the occurrence of typical pernicious anemia has been mentioned. When the developmental defect (or constitutional dyscrasia) is associated with toxemia of a hemolytic type and with the lack of some nutritional factor necessary for the development of normal blood cells, pernicious anemia becomes developed. Improvement often follows relief of the toxemia. Improvement often follows the administration of the lacking nutritional elements. Remissions may be greatly prolonged in either case, but since the constitutional defect is necessarily unmodified relapses are practically certain to occur. Whether modern methods of dietetic treatment of pernicious anemia can prolong the intermission or remission indefinitely remains to be seen. Under older methods of treatment the remissions have lasted for many years, but unless some other disease or some accident causes early death pernicious anemia inevitably returns. The attacks tend to increasing severity and the patient finally dies from pernicious anemia. PLATE VII
K-9. Man forty-four years old. Symptoms indefinite, patient is weak and pale and skin presents peculiar lemon-like tint. At first examination the following blood report was made: Hemoglobin 75.7 gms. per liter (von Fleischl-Miesher)
55% of normal, for age.
During the six weeks after this examination osteopathic treatment was given which was intended to secure better circulation through the ribs. The diet and hygienic conditions were improved and the symptoms diminished rapidly. (This history antedated the use of liver in the treatment of pernicious anemia.) Six weeks after the first examination the following blood report was made: Hemoglobin 100.5 grams per liter (73% of normal)
Hemoglobin 81.2% 58%
The patient disappeared from observation during the next ten months, after which he returned with a history of varying degrees of weakness and dyspnea. No blood examinations were made during this time. One week later he contracted pneumonia and died within a few days. Necropsy twenty-four hours after death. Lungs showed consolidated areas and pleural adhesions abundant, on both sides, all of comparatively recent date and characteristic of pneumonia. Spleen about three times normal size, soft and friable. Liver about twice the mass and nearly three times the weight of normal. Other viscera showed the findings characteristic of pernicious anemia and of pneumonia. Red bone marrow showed great hyperplasia. Tibia completely filled with red marrow of type characteristic of pernicious anemia. Microscopic examinations of lungs, marrow and spleen. Death due to pneumonia with pernicious anemia also present. W-2. Man about fifty years old. May 15, blood findings
as follows:
Hemoglobin 27.5 gms. per liter 20%
Hemoglobin 23 gms. per liter, 17%
Death occurred two days later. Bone marrow only examined.
Ribs and long bones filled with red marrow, paler than usual, of microscopic
structure characteristic of pernicious anemia.
A very peculiar and interesting phenomenon occurs in the blood of certain Negroes and persons of partly Negro descent, characterized by the appearance of red blood cells having a sickle-shaped form. The cells vary in appearance, and may resemble half-moons, commas, oat-grains, and irregular parts of a circle, as well as the typical sickle. The cells seem to include many normal forms, in the circulation, but they are very delicate of structure and soon tend to the characteristic forms when the blood is prepared for examination. The changes which occur after the blood has been taken under conditions suitable for accurate examination were studied with especial care by Levy in 1929. In our laboratories we have had only a few cases and these were not suitable for special study. The tendency to sickle-cell structure of the red cells is a trait associated with imperfect development of the erythrocytopoietic tissues. Normoblasts, megaloblasts, myelocytes and cells showing basophilic reticulation or punctate basophilia are usually present in the circulating blood. Anemia may be slight or profound. In typical cases the red cell count is between two and three million, and the hemoglobin between 40% and 75%. The color index is between 0.8 and 1.2, in typical cases. The white cell counts vary considerably. Usually there is some leuocytosis. It is difficult to find uncomplicated cases because the anemia itself is rarely the condition which causes the patient to come under observation. Immature and myelocytoid forms are abundant. The condition is rather common among the Negroes in Southern States and in the Negro districts of New York and other Northern cities. It has been described in a very few cases of white people whose family history seems to preclude possibility of Negro blood. This peculiar condition seems to be hereditary as a dominant trait according to Mendels Law. The abnormal condition of the red-cell formation
is present throughout life. When some disease affects the individual the
cells are very seriously affected.
At autopsy the spleen and liver are distended with the abnormal red cells and their fragments. In some cases an abnormally small size of the spleen and the liver with moderate hyperplasia of the red bone marrow has been reported. Fatty degeneration of the heart, liver and other organs has been reported. These are apparently due to the anemia itself. Since the condition is evidently developmental no
treatment could affect it in any adequate manner. As in all other conditions
associated with imperfect development, it is necessary to avoid all causes
of malnutrition or ill-health very carefully in order that the unfortunate
individual may have as good a life as is possible under the circumstances.
In such a case as this the importance of keeping the best possible circulation
and nutrition of the red bone marrow is apparent. No cases have been reported
under osteopathic observation and treatment.
In this country chlorosis has almost disappeared during recent years. Chlorosis is a peculiar form of anemia which occurs in girls during adolescence and which has its basis in a developmental anomaly. The aberrant development is indicated by an abnormally small heart and by narrow blood vessels; these conditions are sometimes found only at autopsy, but are always present in typical cases. The heart, originally small, is usually slightly dilated and hemic murmurs are present. The bruit de diable is present in typical cases; this is a sound like the humming of a giant top, heard over the base of the great vessels of the neck. These circulatory conditions are due to the abnormal structure of the heart and blood vessels with compensatory phenomena. Other developmental anomalies associated with chlorosis include congenital weakness of the abdominal muscles and the walls of the abdominal and pelvic viscera. Dilatation of the stomach and intestines and ptoses of the abdominal and pelvic viscera are always present in typical cases. The gastric juice shows low or absent hydrochloric acid, and this defect also is developmental. The chest is rigid and rather narrow and the diaphragm is rather high. The respiratory excursion is always very small. These conditions are primarily developmental but are exacerbated by habit. The adolescent phase of the disease is indicated in the abnormal menstruation and the cystic ovaries,--always present in typical cases. In this connection the occurrence of ovarian cysts and of other developmental anomalies of the ovaries in the female progeny of lesioned animals in the Sunny Slope Laboratories is of interest. In the human race other causes of developmental aberrations are often present, as well as bony lesions in the parents. During the years since about 1890 there has been increasing interest in the care of pregnant women, and osteopathic views as to the importance of bony lesions in the etiology of gynecological and obstetrical complications have been increasingly recognized. The diminishing occurrence of chlorosis is, no doubt, associated with the diminishing occurrence of other developmental anomalies among the more intelligent members of the human race. During the same years also there has been increasing interest in diet, and improved transportation facilities have made possible a supply of fresh vegetables and fruits throughout the entire year. These conditions may be important in the diminishing occurrence of chlorosis. Menstrual disorders are sometimes of the type usually called nervous. Amenorrhea is the most common condition and this is often thought to be a result of the anemia. Dysmenorrhea is also very common. Menorrhia and metrorrhagia are much less common in chlorosis, and the anemia associated with these conditions is typically secondary in nature. That the absence of the internal secretion of the ovaries is not the essential cause of chlorosis is evident from many facts,--chlorosis does not occur before the onset of puberty nor after the menopause under any normal or abnormal conditions; in the days when ovariotomy was a common method of treatment for young women with neuroses or with dysmenorrhea chlorosis did not result (though other serious symptoms did occur), and in laboratory animals the removal of the ovaries does not cause any of the characteristics of chlorosis. With further development of the chlorotic girl, abnormal phenomena of the nervous system are inevitable in typical cases. Behavior becomes increasingly aberrant. Abnormal cravings become manifest; the girl eats clay, charcoal, chalk and other improper articles; she sleeps poorly and wanders around at night; she is furiously in love or as furiously antagonistic to her associates, her teachers, and members of her own family, whether male or female. This abnormal behavior has its basis, no doubt, in developmental anomalies of the nervous system as well as in the abnormal state of the internal secretions of the ovaries and related glands. Headache, neuralgia, cold hands and feet, irregular feverish attacks, and constipation are common symptoms. Dermatographia and other hysterical phenomena occasionally appear. The chlorotic girl is usually fatter than normal. This condition is often only apparent and is due to edema of the tissues. There is, however, some excess of fatty tissue due to deficient oxidation. Imperfect oxidation is inevitable with the low hemoglobin and inefficient cardiac activities associated with chlorosis, but the abnormal state of the internal secretions, especially of the ovary and the thyroid, are also concerned in the abnormal tissue metabolism. The greenish tint of the skin is characteristic. The cause of this color has not been determined. The urine is not of abnormal tint and the conjunctivae are never dark in color in typical cases. The eyes are commonly of great brilliancy, with sclerae rather bluish white. In some cases considerable dilatation of the blood vessels of the skin masks the greenish tint. The lips and the lobes of the ears are yellowish and somewhat waxy in appearance in typical cases. The blood changes are pathognomonic. The hemoglobin is very low, usually between 20% and 40% of the normal for the age of the girl. The red cell count is high, often exceeding the normal. The color index is lower in chlorosis than in any other disease, often being below 0.4, and occasionally reaching 0.25 or lower fractions. Viscidity, alkalinity, specific gravity and osmotic tension are lower than normal. The blood coagulates more rapidly than normal, and this causes a peculiar phenomenon which is rarely present in other conditions. When a drop of blood is allowed to fall upon filter paper, as in making the hemoglobin estimation by means of the Tallquist scale, the plasma spreads into the paper leaving a drop of brilliant red blood, often clotted, in the center of the moistened circle. This increased coagulability of the blood is probably responsible for the thrombosis and sudden deaths which occasionally occur in chlorosis. The total blood volume is somewhat increased. The cell volume is diminished. Poikilocytosis is more marked in chlorosis than in any other disease. Large, pale, edematous cells are conspicuous in the warm-slide examination. True megalocytes are not present. The red cells are very unstable, so that poikilocytosis is much less marked if the blood is taken with great care to avoid distortion; it is very difficult to avoid some distortion of the red cells even in the warm-slide preparations. Immature forms of the cells are abundant. Polychromasia, basophilic reticulation and stippling and Normoblasts are common. Megaloblasts and erythroblasts are not found in uncomplicated cases (Plates I, V, VI) The leucocyte count is normal or low. High counts suggest some complicating disorder. Chlorotic girls react to relatively mild causes of anemia or leucocytosis rather extravagantly. In uncomplicated cases, the lymphocyte count is relatively high and immature forms are common; this relation is of developmental type. Atavistic cells are rare. Neutrophiles are often fragmented they are fragile and easily distorted in preparing the blood for examination. Edematous forms are often noted. Staining reactions vary considerably in different cells in the same smear. The nuclei usually stain feebly. Eosinophiles with abundant, hyaline, basophilic, intergranular protoplasm, large round nuclei and rather large scanty granules are often found. Coarsely granular basophiles and basophilic myelocytes are often abundant. The course of the disease varies. Usually recovery is slow even with correct osteopathic treatment. Under old-time methods improvement is apparently due solely to the development of the girl during the later years of adolescence. Osteopathic treatment has given excellent results. Such treatment is devoted to the correction of the thoracic and upper lumbar lesions usually present, and to securing as nearly normal hygienic conditions as possible. During adolescence some correction of developmental defects seems possible. In many cases compensatory hyperplasia of the heart and increased tone of the muscular walls of hollow viscera are associated with increased hemoglobin content of the blood and practically complete recovery as a result of osteopathic treatment with wises dietetic and hygienic teachings. Girls who do not receive such treatment may seem to outgrow the disease during the adolescent years but the blood continues to show chlorotic traits as long as they live. During their later life any conditions causing anemia causes also a return to the chlorotic type of blood. In one of our cases chlorotic blood appeared in a woman of thirty-five after labor. She had had chlorosis during her adolescence, had apparently recovered from this within a few years and had married at the age of twenty. She had borne three children with no abnormal symptoms. She had borne no children for nine years at the time of the birth of her fourth child. There had been a rather severe post-partum hemorrhage, and the secondary anemia due to the hemorrhage was typically chlorotic in nature. Another patient was forty-six years old. She gave a history of green sickness during her adolescent years, with recovery during the early twenties. She did not have the exact years at which the disease had begun or ended. After the age of twenty-four years she was well and showed no evidence of anemia. Blood examinations made during the thirty-sixth year, at which time she was in the hospital for total hysterectomy following the discovery of multiple fibromata, showed no evidence of anemia. When she was forty years old she suffered a severe attack of acute articular rheumatism and after that she became anemic. At the age of forty-three she came to the osteopathic clinic for examination, and the blood showed a typical picture for chlorosis. |
{kind=link}
{kind=link}