
| The relations between the different classes of white blood cells are not yet satisfactorily determined. The simple cellular relations of the classes of leucocytes found in normal, adult, human blood are quite different from the complicated relations of the blood cells in abnormal conditions of adult blood and in normal conditions of early embryonic development. In normal, adult, human blood the white cells are divided into two distinct groups, the granular cells and the hyaline cells. The granular cells are derived from red bone marrow, during adult life. They are distinguished by the presence of granules within the protoplasm. The hyaline cells do not, normally, show any granules within their protoplasm by ordinary methods of staining. A very few granules may sometimes be brought into view by certain staining methods, but these are scanty and are not distinctive by ordinary staining of normal blood. The hyaline cells are mostly derived from lymphoid tissues and are called lymphocytes for that reason. Granular cells include neutrophilic, eosinophilic
and basophilic, named according to the staining reactions of the granules.
Hyaline cells include large and small, named according to size. Even in
normal blood a few hyaline cells of intermediate size may be found, and
these are increased under abnormal circumstances.
Neutrophiles are white blood cells whose protoplasm is filled with fine granules which are neutrophilic or feebly eosinophilic, and whose nuclei are of extremely variable form. They are about ten microns in diameter in the living state. They have a very delicate intergranular hyaline protoplasm, and this is feebly basophilic. Neutrophiles make up sixty to sixty-six per cent of the leucocytes in normal, adult, human blood. Their number is subject to marked variation under varying physiological states, and still more marked variation under abnormal conditions. They are normally present only in the blood stream and bone marrow, not in the tissue spaces. (Plates III, IV) Neutrophiles are formed only in the red bone marrow,
during normal, adult, human life. Under certain abnormal conditions they
may be formed in the spleen and, probably, in other lymphoid tissue.
The granules of neutrophiles vary somewhat in their staining reactions. Even in a single cell some granules are less eosinophilic than others. In a smear certain cells may be more or less eosinophilic than other cells, and in smears made from the blood of the same normal person at different times there may be greater or less affinity for various stains. As a rule, the physiological conditions of fatigue, hunger and lowered blood pressure cause increased affinity for eosin and similar stains (usually called acid-stains) while exercises, hot baths, deep breathing and other conditions which cause moderate physiological leucocytosis cause also diminished affinity for eosin and increased affinity for methylene blue and other stains usually called basic. The intergranular protoplasm may become definitely basophilic under such circumstances. Since younger forms of neutrophiles show greater basophilia, it is quite probable that the increased basophilia under such conditions is due to the associated leucocytosis. The thin, hyaline, intergranular protoplasm remains present but is not usually visible in the normal adult stained cell. This thinner material seems to be the active part of the cell in ameboid movement, and the pseudopodia as first formed are composed of it. The granules follow in a massive sort of motion, and as they move they maintain a sort of united relationship. (One observer said that they looked as if they were chained together as they marched along.) In this respect the activity of the neutrophile differs from the activity of the eosinophile. In the younger forms a centrosome is occasionally present. The younger forms also often contain mitochondria; these disappear gradually with increasing senility of the cell. The abnormal neutrophilic cells found in leukemia contain peculiar rod-like masses of irregular contour; these may be mitochondria. They may take neutral, acid or basic stains. The relations between these bodies and the true neutrophilic granules have not yet been determined. The granules are very small in normal neutrophiles,
but in excessive fatigue and under pathological conditions larger granules
may be found within the neutrophiles; these may be intensely basophilic,
eosinophilic or amphophilic, or they may retain their normal neutrophilic
or feebly acidophilic affinities. These atypical granules are never found
in normal blood.
The nuclei of neutrophiles present great variations even in normal, adult, human blood. Mononuclear neutrophils have, as the name indicates, a single round or roundish nucleus. This nucleus is centrally placed and it may be slightly indented or reniform. The granules are finer than those of the polymorphonuclear neutrophile and are definitely neutrophilic, very rarely even feebly eosinophilic or acidophilic. The intergranular protoplasm is rather more definitely basophilic and is often more abundant than in the polymorphonuclear forms. Intermediate forms exist between the mononuclear neutrophiles and the polymorphonuclear neutrophiles, and there is some reason for believing that the mononuclear cells are immature forms of the polymorphonuclear forms. Nuclear structures take the basic stains with avidity. One or two nucleoli may be present. The nucleus of the polymorphonuclear neutrophile presents great variations both in normal and in abnormal blood. Neutrophiles with deeply notched or saddle-shaped nuclei are grouped with the polymorphic forms. Nucleoli are rarely found in the younger forms, and are never found in older types. Apparently with increasing age of the cell, the nucleus becomes more and more slender, finally approaching the form of a ribbon or a cord, folded back and forth in a very irregular manner. This ribbon-like structure may be variously indented and the wider portions may be connected only by fine threads of nuclear substance. Rarely these lobules may be completely separated; at least, no nuclear substance connecting them can be demonstrated by ordinary staining methods. In normal blood the number of distinct lobules rarely exceeds four; in abnormal blood there may be six or even ten or more distinct lobules in a single cell. These nuclei do not show such distinct structure as is found in the mononuclear forms. Cells with the greatest number of nuclear lobules show the greatest senility in the character of the nuclear structures. The chromatin is in large irregular masses and is avidly or feebly basophilic. When marked toxemia is associated with neutrophilic proliferation some of the cells may show abundant senile traits while other cells show marked evidences of immaturity or even of atavism. The staining reactions of the nuclei as well as the
number of nuclear lobes or lobules vary with changing physiological conditions.
In pathological conditions these variations may be extreme. When there
is increased outpouring of neutrophiles from the red bone marrow under
physiological conditions, such as the increase which occurs as a result
of rapid traveling to high altitudes, many young forms are found in the
peripheral blood. These young forms show larger nuclei with fewer lobes,
simpler forms and more delicate nuclear structure than do the older forms.
The cells thus thrown into the peripheral circulation are so speedily produced
that they must have been already formed and held in reserve in the sinuses
of the bone marrow. They do not differ from the younger forms of the cells
previously in the circulation, the only difference being that there are
many more of the younger forms than is ordinarily the case. Within a day
or at most a few days the cells become older and the blood picture is practically
that of the individual before his journey.
Under certain abnormal conditions the neutrophiles are manufactured more rapidly than is normal, and very immature cells may be thrown into the general circulation. These include myelocytoid forms and myelocytes. The nucleus is very large and occupies more than half the entire area of the cell; it is round or roundish, is eccentric as in its position and is often bare of protoplasm upon one side. It has one to three nucleoli which stain deeply. The chromatin is fine and deeply staining and is arranged in irregular masses. These cells are abundant in cases of myeloid leukemia and may be found in considerable numbers in cases of severe, acute, pyogenic infection. With still more rapid formation of leucocytes, especially
when the hematopoietic areas approach exhaustion, atavistic types are occasionally
found. These cells are not present in normal adult human blood or marrow.
Atavistic forms are occasionally found in abnormal embryonic human blood
and in abnormal adult marrow, but they are characteristic of the cells
of mammals below human, or of vertebrates below mammals. The neutrophiles
of human blood are not exactly like those of other mammals, and no cells
which can properly be called neutrophiles are present in the blood of animals
below mammals. For this reason it is easier to recognize atavistic forms
among the neutrophiles than it is to find them among the hyaline cells,
because the latter are found in about the same forms in all mammals and
in nearly all vertebrates. (Plates V, VI, XII)
Bony lesions affect the structure of the neutrophilic cells recognizably. Any bony lesion is associated with a disturbance of the circulation through the red marrow of the bones concerned in the lesion and, in the case of small bones, those in the immediate vicinity of the bones actually concerned in the lesion have also some circulatory disturbance. For example, when one rib is lesioned there is some edema of the tissues around the joint or joints concerned in the lesion. This edema frequently extends beyond the nutritive foramina of neighboring ribs as well as those of the rib which is lesioned and often also to the foramina of adjacent vertebrae. The nerves and blood vessels passing through these nutrient foramina are subjected to the pressure due to the edema. The nerves, especially those which are non-medullated, are subjected to the chemical changes in the edematous tissue juices. Because of these physiological relations, the red marrow of one or several bones has some circulatory disturbance whenever there is a bony lesion anywhere in the body. The red marrow thus affected produces blood cells which are not quite normal in structure; such cells are usually immature or myelocytoid in type; the nuclei are roundish, somewhat vesicular in form, show larger and paler chromatin masses and occasional nucleoli. Their protoplasm shows granules of irregular size and irregular staining reactions. The intergranular hyaline protoplasm is more abundant. These cells flatten to a thinner layer on the slide than do normal cells, and their pseudopodia are less regular in form, are protruded from two or several parts of the circumference of the cell simultaneously and are less efficient in the ingestion of bacteria or of foreign particles than are normal pseudopodia. The presence of these immature or myelocytoid forms,
in blood which shows no other cause for this abnormality, indicates the
existence of some conditions causing inefficient circulation through the
red bone marrow somewhere in the skeleton. Bony lesions are the most common
cause of such nutritional defect of the red marrow.
Arneths index is the result of computations based on nuclear structures. It is supposed that those neutrophiles which have a single nucleus, round or only indented, are the younger forms. Those with two lobes are younger than those with three lobes. In the older neutrophile the nucleus is almost or quite divided into several lobes. Arneths index is a method of estimating the relative age of the neutrophile by means of a study of these variations in the nuclear structure. While the nuclear lobulations may not be altogether accurate as a basis for the calculation of age, still this study gives useful results under certain conditions. In our laboratories Arneths index has been superseded by a study of the neutrophilic nuclear average which we find much more useful. (Plates XIV, V, IV) Arneth divided the neutrophiles into five groups, Class I having a single nucleus which is round or indented; Class II having two nuclei, and so to Class V which has five or more nuclei. Each class is subdivided according to the form of the nucleus. In Class I are three groups, M cells which are really myelocytes and are not found in normal blood; W cells which are mononuclear neutrophiles or myelocytes and have nuclei which are slightly indented or reniform, and T cells which have nuclei rather deeply indented but which are still definitely single in structure. The W cells may or may not be found in normal blood and, if present, are very scanty. T cells may make up 5% of the total neutrophile count. Classes II, III, IV, and V are subdivided into different groups according as the nuclei show definite knob-like lobes, or are ribbon-like with grouping of chromatin in such a manner as to form lobules. Both forms of nucleus may be present in a single cell, so that Arneth describes in Class II cells with two knob-like projections, cells with two S-shaped masses, and cells with one S-shaped lobe and one knob-like lobe. Class II has, altogether, about 35.5% of all neutrophiles, in normal blood. Class IV has four subdivisions, based on different combinations of the knob-like and the S-shaped nuclei, and this class makes up about 36% of all neutrophiles of normal blood. Class IV has five subdivisions and makes up about 2% of all neutrophiles in normal blood. These percentages are given from various laboratories and they are practically identical with our own figures. According to Arneth, the neutrophiles are greatly increased during infections and hence immature forms are found in the circulation; the index is then said to shift to the left, that is, there are many more cells in the first and second classes than is the case with normal blood. After an infection has been present the younger cells are no longer being formed so rapidly, there is an accumulation of older forms, and an increased number of cells in the fourth and fifth classes. However, the effect of toxins on the white cells also increases the number of nuclei, causes the nuclei to become pyknotic and the chromatin to become arranged in irregular masses. Fragmentation, vacuolization and cloudy swelling of the protoplasm, with a loss of the distinctive granules, lead to great difficulty in estimating Arneths index in many cases, and especially in those cases in which the diagnostic value of the method is of most importance. Modifications of the method of determining the index of Arneth have been devised by Cooke, Schilling, Ponder and others. After considerable study of normal and abnormal bloods we have discarded all of these in favor of the study of the neutrophilic nuclear average. In making this computation true myelocytes are disregarded and only typical mononuclear and polymorphonuclear neutrophiles are included in the count. The myelocytes, if present in any considerable numbers, are separately estimated. In this method the myelocytes which are present as a result of imperfect circulation through the red bone marrow, or of developmental abnormalities, or in the blood of leukemic patients, are not allowed to affect the nuclear average. Thus the nuclear average represents only the relative ages of the neutrophiles. In this connection it must be remembered that toxemias often increase the nuclear average and cause, in other ways, an appearance of senility in neutrophiles. Arneths index shows marked shift to the left (predominance of youthful and immature forms) when there is efficient reaction to acute infections; pneumonia and pyogenic infections generally cause extremely marked shifting. During an infection to which the myeloid tissues do not make adequate response, toxemia is severe, the neutrophiles show abundant senility and there are relatively very few young cells being thrown into the circulation; the index is shifted to the right in such a case. After an infection and during recovery there is also a shift to the right, due to the fact that young cells are not being thrown into the circulation and the cells already present are somewhat affected by the toxemia of the infectious processes. There is a marked shift to the right in jaundice, in toxemias due to malignant neoplasms, the absorption of old pyogenic foci or degenerating benign neoplasms, in intestinal toxemia due to putrefaction and in many other conditions associated with disturbances in putrefactive products anywhere in the body. The changes in the nuclear average are of similar import. The normal adult neutrophili nuclear average varies from 2.45 to 2.55. During the early stages of an acute infection this decreases to below 2 and occasionally to 1.5. The nuclear average is below 2.3 in normal young children and may be below 1.3 during an acute infection in childhood. In chronic toxemia and during convalescence from
an acute infection the nuclear average often exceeds 3.0 and in senility
it is normally above 2.7.
The lower the neutrophile nuclear average, the greater
the proportion of newly-formed, young neutrophiles; the higher the average,
the greater the proportion of worn-out and elderly neutrophiles.
The functions of the neutrophiles have not been adequately determined. That they are important factors in protecting the body against certain types of bacteria is evident, though they are not efficient in other infections. They ingest and digest and render harmless injured tissues and many foreign substances within the body. The fact that they increase and diminish so rapidly at different times of the day and, under certain circumstances, during the digestion of food leads to the view that they may have a nutritive function. In their own metabolism they take up nitrogenous substances and, probably, certain forms of carbohydrate related to glycogen. When they die and are digested and absorbed and, perhaps as a result of their own living metabolism, these substances are given off again into the blood plasma. They represent a storehouse of food materials and are very efficient in this relation, since substances so stored do not affect the composition of the blood plasma, and since they are so thoroughly scattered over the body that they are immediately at hand for every demand. They carry tiny globules of fat in their protoplasm, and this also is an efficient method of storage. They elaborate an enzyme which is efficient in the
digestion of necrotic tissues resulting from injury of the body cells and
from exudates, transudates or hemorrhages within the body. After pneumonia,
for example, the processes of resolution are due chiefly to the activities
of the leucocytes and of the enzymes formed by them.
The neutrophiles are normally formed, during adult life, only in the red bone marrow. From the stem cell arise myeloblasts which show differentiation by the development of individual cells and as a result of the unequal division of the mother cells. The myelocyte of the neutrophilic series is a large cell with its nucleus occupying much more than half the mass of the cell. The protoplasm is very finely granular and many contain mitochondria; it is feebly basophilic. With further differentiation the nucleus becomes smaller and the protoplasm more abundant; the nucleus loses its nucleoli and becomes lobed; the protoplasm loses its nucleoli and becomes lobed; the protoplasm loses its mitochondria and developes more abundant granules which become more and more definitely neutrophilic. The protoplasm is pushed or grows toward the endothelium of the blood vessels of the marrow, and finally it enters the blood vessel through the endothelial wall. In human marrow there are many spaces in which no endothelial wall can be seen; the cells are simply pushed out into the blood stream. Under normal circumstances only the myelocytes of
almost adult type seem to be concerned in reproduction; at any rate karyokinesis
is seen only in those cells in normal, or almost normal, human marrow.
In the leukemias and in pernicious anemia karyokinesis is abundant among
the earlier myeloblasts and also among the stem cells.
The length of life of the neutrophiles cannot be estimated in any satisfactory manner. The rise of the nuclear average during a few hours after an acute leucocytosis due to acute infections would seem to indicate that the development of young to senile forms is rather a hasty process under such conditions, which are, of course, distinctly abnormal. Neutrophiles containing carbon particles may be found several weeks, even several months after such particles have been injected into the veins, but these same particles may have been ingested and left behind at the death and digestion of many cells in the interim. Cells which appear to be senile are found constantly
in normal blood. They fail to show normal movements on the warm slide;
they do not stain distinctly; they have swollen and fragmented nuclei and
swollen and fragmented protoplasm. Naked or almost naked nuclear masses
of distinctly neutrophilic type are found and the occasional ragged fragments
of protoplasm which may occasionally be found clinging to such nuclei are
of neutrophilic structure. In the blood of a normal young woman such cells
were found to be present, in the early morning, 25 senile cells or naked
nuclear masses to 230 normal neutrophiles. At nine oclock at night 25
senile cells or naked nuclei were present in 150 normal neutrophiles. Other
estimations of this relation in several other apparently normal persons
gave similar results; in some cases the differences between morning and
evening blood were much greater. Based upon these studies, the life of
the neutrophile in circulation can scarcely be more than a week. Estimations
based upon the increase present in infections give one day or two days
as the probable life period of the neutrophiles.
Fragments of leucocytes are found in the endothelial cells of the spleen and the liver, and, to some extent, of the bone marrow. These are, no doubt, utilized as food by these and perhaps other cells of the body. The molecules of which they are composed seem to be very well adapted to serving as food for other cells, and it is quite probable that in building up the food materials brought into the body into these more complicated molecules they serve their most important physiological function. Eosinophiles are, as the name indicates, intensely eosinophilic or acidophilic. A typical eosinophile is about 9 microns in diameter on the warm slide. From .5% to 1.5% of the total leucocyte count are eosinophiles in normal adult human blood. In children the number of greater both relatively and absolutely. Under certain abnormal conditions of adults and children the number may be very greatly increased, even to 80% of the total leucocyte count. Nearly all animal blood contains higher eosinophile counts than human blood, and young animals show higher eosinophile counts than do older animals. Eosinophiles show hyaline protoplasm filled with
very large granules. These are conspicuous objects on the warm slide. When
they are stained with eosin they are very brilliant and noticeable. In
younger cells and in eosinophilic myelocytes the intergranular, hyaline,
basophilic protoplasm is visible. In older cells this protoplasm can sometimes
be demonstrated by very delicate staining methods. The granules seem to
be definitely alive; they are the active elements in the movements of the
cell.
In lower mammals the granules are often definitely oval or rod-shaped. The rod-shaped form occasionally appears in human blood when other atavistic characteristics are present. The oval form has not been reported in human blood. The nuclei vary in form, but are always roundish
in outline. Reniform and saddle-shaped nuclei are common forms. They are
never ribbon-like, nor are they so markedly polymorphic as are neutrophile
nuclei. The nuclei have rather a coarse structure. The chromatin masses
and net-knots are larger than in hyaline cells and are not so deeply basophilic.
Dividing forms are not seen in normal human blood, but under abnormal conditions
in human blood, in the blood of embryos and in lower vertebrates dividing
eosinophiles are occasionally found. Nuclear pseutopodia are never seen
in normal blood, either animal or human, and are rarely found in abnormal
blood.
Eosinophiles move with considerable celerity on the warm slide. They die within twenty or thirty minutes. The large granules are the active element. One granule usually begins to roll over; this may be near the nucleus or at the periphery. It rolls over and over, between or over other granules but not necessarily causing these to move. Other granules then begin to move and these tend to follow one another in curving lines. Very often these curved lines of granules are discernible in the stained cell. The hyaline part of the protoplasm, when it is visible, usually follows the granules. Occasionally, especially in the blood of fasting patients or those with severe malnutrition from any cause and in very young or animal blood, the hyaline substance may precede the granules and the granules may even, sometimes, seem to be carried along by the streaming protoplasm without displaying any intrinsic activity of their own. The nucleus follows the protoplasm sometimes, and it seems to be carried along as if it were heavy or reluctant. In many cases the nucleus does not move at all; the granules flow away in long masses, sometimes leaving the nucleus almost or quite naked, then they return to surround the nucleus almost evenly; they may then flow out in another direction only to repeat the process. This phenomenon is most commonly seen in blood which has been taken from a feverish patient, or in blood which has been under observation upon a slide whose temperature is one or two degrees above that of normal blood. Phagoytosis has not been observed in eosinophiles though their ameboid movements are so rapid. (Plate II)
Very little is known of their functions, and a study of the conditions associated with their increase and their decrease add little to our understanding. The granules contain iron and copper and they seem to be concerned in iron and copper metabolism. They are very abundant in the sputum under certain conditions. The formation of Charcot-Leyden crystals and crystals of the seminal fluid is usually associated with their degeneration. Eosinophiles are diminished in nearly all uncomplicated acute pyogenic infections. A differential count of 5,000 leucocytes made for one of our cases with lobar pneumonia included no eosinophiles. After the crisis in pneumonia and after the fall
in fever in most acute infections the eosinophiles increase rapidly, often
considerably exceeding the normal numbers.
Eosinophilia, or marked increase in the eosinophiles, occurs under many different physiological and pathological conditions. Eosinophiles above 2% should be considered a relative increase and above 200 per cubic millimeter an absolute increase, but the term eosinophilia is usually employed only when the eosinophiles rise above 3%, relatively, and above 300 per cubic millimeter, absolutely. Eosinophiles are increased physiologically during and for a day after physiological congestion of the reproductive tissues, that is, after sexual excitement in both sexes, and before menstruation in women or at the time of heat in female animals. They are also increased as a result of vertebral lesions which cause congestion of the reproductive glands; this is more marked in the female with congestion of the ovaries produced by lesions than in the case of the male with congestion of the testes as a result of lesions. Correction of lesions concerned is followed by decrease in the eosinophiles within three days, in human subjects. They are increased in diseases of the spleen, including the congestion of the spleen due to lesions of the ninth thoracic vertebra, and, in less marked degree, of neighboring vertebrae and ribs. Diseases of other lymphoid tissues do not cause eosinophilia in the same degree, nor is it always present. After splenectomy and after destruction of considerable splenic tissue by neoplasms eosinophiles are increased also. In cases of splenomegaly the eosinophilia may reach tremendous heights. Counts exceeding 80% of the total leucocyte count and 130,000 per cubic millimeter absolute count have been reported by several workers. Diseases of the bone marrow, including myelogenous leukemia, usually show high actual counts of eosinophiles, often exceeding 20,000 per cubic millimeter. In osteomyelitis, osteomalacia, sarcoma and carcinomatous metastases and in less common diseases of the bone marrow the eosinophiles may be greatly increased. In pernicious anemia they are relatively increased and they may be absolutely increased even though leucopenia may be extreme. The absorption of the toxic products of degeneration of animal proteins causes eosinophilia, but the absorption of degeneratiang vegetable proteins does not. In intestinal putrefaction the eosinophiles are increased if the patient is on a diet high in meat or eggs, but not if he is on an exclusively vegetarian diet. Mild eosinophilea is present in malaria, syphilis and during the absorption of exudates, transudates, and pus, and during resolution after pneumonia. It is often present when degenerating benign neoplasms or rapidly growing malignant neoplasms are present in the body. Eosinophilia may be marked during the fever of scarlet fever, measles and acute articular rheumatism. In cases of mumps with overitis or orchitis the eosinophiles are increased, and this rise may precede recognizable symptoms of the spread of the inflammation to these tissues by a day or even two days. The value of this reaction is evident. Eosinophilia may be marked after the use of any of the animal substances used in the treatment of disease, such as tuberculin, antitoxin and vaccines. They are not increased after the injection of vegetable proteins unless anaphylaxis or definite irritation of the skin is associated with the injection. They are occasionally diminished immediately after the injection of animal products, then rise to a surprising degree within a few hours; counts of 40% and of 45,000 per cubic millimeter have been reported. Eosinophilia in bronchial asthma is useful in differentiating bronchial asthma from symptomatic dyspnea. It must be remembered that the eosinophiles are also usually increased in emphysema. In uncomplicated bronchial asthma eosinophilia is always present, usually above 8% of the total leucocyte count and above 1,000 per cubic millimeter of blood in our cases. Diseases affecting the sympathetic nervous system may cause marked eosinophilia; this is especially noted in cases in which the solar plexus is invaded by carcinomatous metastases. Any irritation of the skin causes increase in the eosinophile count, whether this be mere mechanical or chemical irritation or whether inflammation of the skin is present (as by poison oak). Even rather small burns may cause marked eosinophilia; it may be that the absorption of the proteins from the injured tissues is a factoring this case. Counts up to 60% of total leucocyte count, and to 4,000 eosinophiles per cubic millimeter of blood have been reported in urticaria; with relief of the hives the eosinophile count returns to normal within a few days. Any skin disease associated with itching or other sensory irritation increases the eosinophiles to some extent, and this increase may be surprisingly high for mild cases. There seems no relation between the area of skin involved, the severity of the disease or of the sensory irritation and the height of the eosinophilia. Animal parasites usually cause definite or high eosinophilia. Amebic infections frequently cause no eosinophilia at all, and in uncomplicated cases there is never more than a slight increase in eosinophiles. Filaria sanguinis hominis usually is associated with mild eosinophilia. Darlings hisoplasma capsulata caused slight eosinophilia in the one case studied in our laboratories. Hydatid cysts of the liver may cause little or high eosinophilia, usually less than 20% of the total count. Trichinae cause eosinophilia which may be of diagnostic value in obscure cases of muscular pain. Worms in the intestinal tract often cause very high eosinophilia, to 70% or even more, and to 8,000 eosinophiles per cubic millimeter of blood; commonly the count runs from 15% to 25% for the ordinary pinworms, round worms and tapeworms. Several drugs may cause eosinophilia, usually moderate and transitory. Camphor is of interest in this connection and persons whose occupation causes the inhalation of camphor fumes may show persistent eosinophilia. Diagnosis is sometimes difficult in such cases. It is evident from this review of the changes in
eosinophile counts that the biology of these peculiar cells is extremely
complicated and that much further study must precede our satisfactory understanding
of their behavior under normal and abnormal conditions.
Normal human adult blood occasionally shows eosinophiles in which the nucleus stains feebly and the granules are separated widely. These cells are undoubtedly disintegrating. Such cells are much more abundant in abnormal blood. Fragments of these cells can be found within the cells of the spleen and the liver, and in other areas of the reticulo-endothelial system. In abnormal blood they are occasionally found within the endothelial cells. There seems to be no doubt that these cells die in
the circulation, are ingested by phagocytic cells and are used as food
by the tissues of the body.
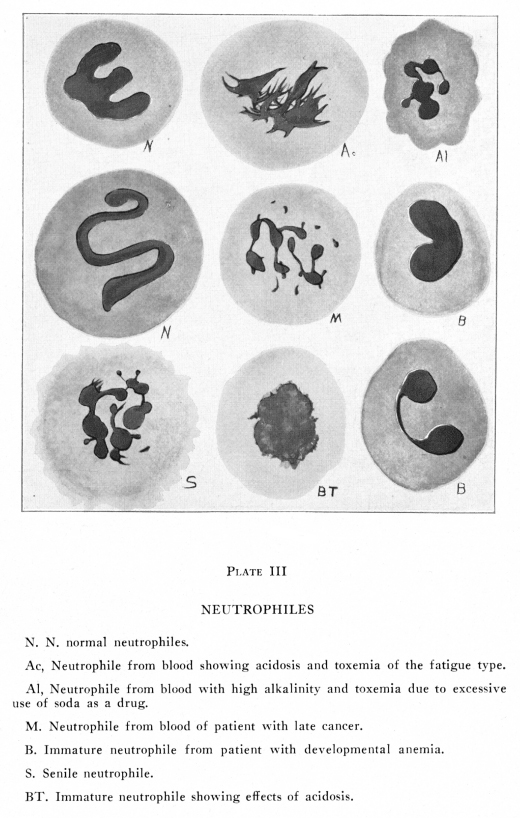
Basophiles, or mast cells, are scanty in normal, adult, human blood, but are more common in embryonic blood, in the blood of animals and during the course of certain diseases, especially the leukemias. In normal adult human blood one or two mast cells may be found in a differential count of 2,000 to 5,000 cells. Occasionally a specimen of normal adult human blood is found which contains no basophiles at all, even when several students make simultaneous differential counts of the same blood taken at the same time, each student counting 500 to 1,000 cells. If the basophiles exceed 1% or 100 per cubic millimeter of blood, some explanation of the excess must be sought. A basophile is eight to ten microns in diameter on the warm slide. It has a nucleus which may be roundish but is usually lobate. The nucleus stains feebly and chromatin masses are usually very dimly visible. There is a very scanty hyaline, feebly, Plate III
Mast cells, or basophiles, give the oxidase reaction. They are formed in the red bone marrow. Cells which are indistinguishable from these except that they may not give the oxidase reaction, are present in the tissues of the body, and these are increased during inflammatory states, especially those of traumatic origin. These cells are known to enter the blood stream and it seems very probable that they wander into and out of the blood vessels according to the changing tensions of the various gases and other substances in solution in the blood plasma and in the tissue juices. They are more abundant in the tissues when absent in the blood, and vice versa. It is not yet known whether they have any functions
different from those of other granular cells or not. They are increased
in the leukemias. In gonorrheal pus and in pleural exudates they are often
very abundant; these abnormal accumulations of basophiles differ somewhat
from the basophiles found in normal blood and also from those of leukemia.
In abnormal blood amphophilic cells are sometimes found. Only rarely do they appear in the blood of healthy individuals. These have usually a single round, vesicular, eccentric nucleus, often lobate, rarely notched or polymorphic, feebly staining with ordinary nuclear stains, and often very eccentrically placed. The granules are vividly stained, some with basic and some with acid stains. These, lying over the paler nucleus, offer a brilliant spectacle. By washing the smear with a feebly acid or feebly alkaline solution, the amphophilic granules can usually be induced to stain as eosinophiles or as basophiles at will. In general appearance the amphophile resembles the basophile, with which it is usually associated. Hyaline cells form from one-fourth to one-third of the white cells of normal adult human blood. Of these the lymphocytes are the most numerous. Monocytes are present in small numbers. Under abnormal conditions plasma cells, hyaline myelocytes and a few other less common forms may appear. In the discussions of these less common forms there have been great differences in the terminology employed by different authors. The developmental relations of different types have also been a matter of considerable discussion, and many disputed points must await further study. In this connection the differences of opinion between the Unitarians, who hold that the stem cell is the progenitor of all blood cells, and the dualists, who believe that there is a limitation of the developmental potentialities of the stem cells, is of some temporary interest. With further study the actual facts will terminate the discussions. The development of certain forms of hyaline cells
from certain other forms is well known. Defibrinated blood containing no
plasma cells, placed in tubes and kept in moist air in an incubator, was
found to contain plasma cells after five days, in our laboratory. In other
laboratories cultures of blood cells have shown various instances of a
changing cell type, apparently due to metaplasia. Studies made of inflamed
tissues indicate that certain cells may become transformed into other forms
under abnormal circumstances.
Normal adult human blood contains small lymphocytes, which make up about 25% of the white cells; large lymphocytes, which make up about 4% of all the white cells; and, occasionally, a cell is found which is intermediate in size between the large and the small lymphocytes. In the lymph nodes there are hyaline cells of very much larger size, the progenitors of the lymphocytes of the blood. These may enter the blood under abnormal conditions and they are then called large endothelial cells or giant lymphocytes according to their stage of development. Lymphocytes are found in relatively larger numbers in the blood of young individuals, whether human or other mammalian blood is studied; and the lower mammals have larger proportions of lymphocytes than the higher. Normal adult human beings have a smaller percentage of lymphocytes than is to be found elsewhere among mammals. (Plates X, XIII) The functions of the hyaline cells are not well known. The large hyaline cells are phagocytic for certain pathogenic organisms, epecially for protozoa (malarial parasites; histoplasma capsulata). Since they are increased during certain infections it may be supposed that they exert some protection against either bacterial invasion or bacterial poisons. The phagocytic activity of the lymphocytes seems to be an important factor in the absorption of fats from the intestinal tract. In this way particles of fat are carried into the lymph spaces without the necessity of first being broken up into soluble substances. They also are concerned in providing conditions necessary for growth and repair. This last function is not well understood. They may neutralize poisons or they may elaborate needful nitrogenous materials for building or they may perform other services. Lymphocytes and other large hyaline cells from the
blood are able to live and to multiply in blood serum, in vitro. Fibroblasts
are unable to grow in blood serum alone, but when cultures of lymphocytes
and large mononuclears grow near cultures of fibroblasts, the latter become
able to live and to multiply. Apparently the lymphocytes produce from the
serum albumins or globulins the substances required by the fibroblasts
for their nutrition. An important function of the lymphocytes is the utilization
of proteins absorbed from the intestinal tract in the manufacture of the
peculiar proteins necessary for the feeding of the other cells of the body.
The lymphocytes of normal adult human blood are formed in lymph nodes and in the spleen, tonsils and other lymphoid structures. These derived from the red bone marrow are from small lymphoid masses within the marrow and not from those areas of the marrow which produce the red cells and the granular cells. A short review of the structure of the lymphoid tissue explains the manner in which lymphocytes are formed and are enabled to enter the blood stream. In the spleen, tonsils and all other lymphoid tissues the structures present similar characteristics. There is a delicate framework of connective tissue trabeculae, and associated with this are the reticular cells. These are stellate, oval, spindle-shaped or elongated cells with a nucleus which is roundish, oval or elongated, and has scanty, feebly basophilic chromatin. These reticular cells are abundant in many organs of the body; they are phagocytic and moderately motile. They are part of the reticulo-endothelial system and share in the general functions of that system. Associated with the reticular cells is a group of cells, usually syncytial, with smaller, paler nuclei, less differentiated protoplasm, and no apparent motile or phagocytic activity. Between the reticular cells and the syncytial cells are all intermediate forms, and the syncytial cells seem able to change into reticular cells or to produce lymphocytes on demand. They are not found in the circulating blood in typical form. The connective tissue traveculae with the histiocytes and the syncytial cells form the reticulum of the lymphoid tissue. In the interstices of this reticulum there are abundant masses of lymphocytes and a varying number of reticular cells (histiocytes or macrophages) which have become removed from the immediate vicinity of the traveculae. The lymphocytes include several sizes. Cells apparently identical with the large lymphocytes of the circulating blood are present. These have been called lymphoblasts or lymphoidocytes in this situation. They are most abundant in proliferating lymphoid tissue and are rather scantily found in resting lymph nodes. They divide by karyokinesis and thus are formed the small lymphocytes. Cells identical with the small lymphocytes of the blood stream and of the tissue spaces generally are most abundant in the lymph nodes. These do not divide. They may be the only cells present in the spaces of the reticulum of a resting lymph node. Very large lymphocytes, never found in circulating normal human blood, apparently are the daughter cells of the lymphoblasts grown to several times their original diameter. They often show karyokinetic figures and their daughter cells are smaller in size; small lymphocytes may be derived from these cells also, especially in rapidly proliferating lymphoid tissue. These very large lymphocytes are never found in circulating normal human blood but under abnormal conditions may reach the blood stream. They are not identical with the giant lymphocytes of the blood of certain lower mammals, sometimes found in the atavistic blood of morons or other imperfect human beings. Cells showing karyokinesis are not found in the blood stream normally, but when lymphoid tissue is seriously inflamed or in lymphatic leukemia dividing forms may be found in the circulating blood. Cell division of lymphoid tissue is always by karyokinesis. Direct division and building have never been reported for them. The tonsils and spleen as well as other lymphoid tissues show peculiar pale, roundish areas called nodules or germinal or germ centers. The general structure of these areas is about the same as that already described, but these centers undergo marked variations in activity, both normally and in answer to unusual demands made upon them by toxic or inflammatory conditions. Each such nodule has its own blood supply and this
may be the only visible indication of such a nodule in the resting lymph
node. No such nodules are present at birth or for some weeks thereafter;
they increase rapidly during childhood and youth, then diminish very slowly
until, in old age, they disappear altogether. They show considerable variations
in activity even under normal conditions, and they react to toxic and inflammatory
states with very rapid proliferation.
During a period of increased proliferation the blood supply becomes increased. Vasomotor nerves for these tissues have not been demonstrated nor are secretory nerves known to exist for them. The impetus to increasing proliferation seems to be in the character of the blood or the lymph reaching the nodes. The node of stimulation is not yet understood. The outlines of the nodule become very definite and they are paler in tint than the rest of the section of a lymph node in all ordinary methods of staining. The reticulum is relatively less abundant but it has the same structure as in other parts of the section. The lymphocytes are usually chiefly of the lymphoblast type and these show abundant karyokinesis. The very large lymphocytic cells are also present; very frequently these are grouped in threes to sixes; rarely in larger groups. Many intermediate sizes are present. Small lymphocytes are occasionally very abundant. Very large reticular cells, macrophages containing fragments of blood cells and lymphocytes, are often present; these are derived from the reticulum in this location as in other parts of the lymph node. They may reach a diameter of twenty or more microns, especially in the lymphoid proliferation due to acute pyrogenic inflammation. A comparison of the resting lymph follicle with those in various stages of activity indicates that the reticular cells in the immediate vicinity of the arteriole supplying the nodule first show karyokinesis and that the cells so produced show consecutive changes and differentiation with succeeding divisions and growth until the lymphocytes are produced they tend to assume positions at the periphery of the nodule. As they are small cells with relatively large deeply basophilic nuclei they form a dark ring which seems to surround the nodule. They pass from this peripheral location into the lymph stream and the venous blood. As they increase slightly in size in this passing they become the adult small lymphocytes of the blood and the tissues. As the period of activity wanes the peripheral zone of small lymphocytes forms a smaller and smaller ring around the diminishing numbers of larger, actively dividing cells until these have almost disappeared and the nodule again assumes its resting stage. The small lymphocyte has about the size of an erythrocyte, in life, but it may spread out to eight or nine microns in diameter in a thin, stained smear. The protoplasm as seen in the living cell is almost or quite structureless. By special methods of staining a few azur granules and a delicate cytoplasmic reticulum can be made visible. The cytoplasm varies from deeply to faintly basophilic. There is no cell wall and the limiting layer is of the sol type. In many cells there is so thin a layer of protoplasm that the nucleus may seem to be almost or quite naked. Mitochondria are small and lie near the nucleus. The protoplasm is somewhat more abundant upon the side of the cell opposite the crease in the nucleus. The nucleus has a limiting layer which is quite distinct,
and a nuclear wall is sometimes discernible. The nuclear structures are
deeply staining. One rather large and two or three smaller nucleoli are
usually visible. The chromatin is arranged in rather large irregular masses
presenting something of a tiger-skin arrangement. Wheel-like arrangements
are rare. The nucleus usually shows a shallow or deep groove or infolding
upon one side.
The large hyaline cells of normal, adult, human blood are ten to twelve microns in diameter, in the living state, and they make up from four to eight per cent of the white blood cells. They are relatively increased by those physiological conditions which diminish the neutrophiles, but are not actually increased by physiological conditions. Under certain abnormal conditions they are considerably increased. They are relatively decreased by those conditions which cause actual increase in the neutrophiles and other cell elements but are not actually diminished appreciably under any normal conditions. In large lymphocytes the protoplasm varies in basophilia and granules are stained with more difficulty. The cytoplasmic reticulum is more easily demonstrated. The edges are even more definitely of the sol type and the periphery of the cells seems to pass indefinitely into the blood plasma in cells which seem to be older. These cells are phagocytic and they ingest animal parasites of the blood with avidity. The nucleus is not often moved about by the ameloid activity present on the warm slide. The cytoplasm contains azur granules and occasionally, a few basophilic granules of varying degrees of basophilia. Mitochondria are somewhat more abundant than in small lymphocytes. On the warm slide the protoplasm may form bud-like pseudopodia which become detached from the cell completely. The nucleus is almost spherical and it has a fold
or crease actor one side. In some cells this fold may divide the nucleus
into two almost separated parts; in other cells the nucleus is only notched,
creased, reniform or saddle-shaped. The chromatin masses are arranged much
as is the case with the small lymphocyte nuclei, and they are about the
same size; there are clear spaces between the chromatin masses and fine
linen threads pass between the chromatin masses. In cells which appear
to be older nuclear vacuoles and canaliculi are often present; these are
filled with a clear fluid which does not take any of the ordinary stains.
The proportion of hyaline cells is increased under many pathological conditions. Physiologically, the hyaline cells are relatively increased by fasting and relatively diminished by the factors which cause an increase in the neutrophiles. They are actually increased at fairly regular intervals corresponding to the periods of increased proliferation during the active phases of lymphoid tissues. Emotional states suddenly produced increase the leucocytes, especially the hyaline cells, temporarily. This reaction does not occur in animals or human subjects who have undergone splenectomy. Animals which have been subjected to injury of the splanchnic nerves or the solar plexus do not show the reaction. Under the influence of emotions, especially fright and anger, the splenic capsule contracts, thus forcing many hyaline cells into the blood stream. The biological significance of this increase in the hyaline cells lies in the fact that these cells have, as one of their important functions, the healing of wounds. Lymphocytosis, or abnormal increase in the lymphocytes, occurs more frequently in children than in adults. It is usually marked in ordinary gastro-intestinal diseases of children, in rickets, mumps, whooping-cough, bronchopneumonia and cervical adenitis. The lymphocytes are increased also during the reaction to tuberculin used for diagnosis. In severe pyrogenic infections to which the hemotopoietic tissues are unable to react efficiently there may be a great increase in the hyaline cells. They are increased in several adult diseases, such as malaria, typhoid, relapsing fever and a few less common conditions. The large hyaline cells and especially the monocytes are greatly increased in agranulocytic angina, kala azur, Malta fever and also in severe pyrogenic infections when ordinary granular leucocytosis does not occur. The large hyaline cells are increased in tetrachlorethane poisoning. Chronic diseases which are usually characterized by lymphocytosis are syphilis, whether acquired or inherited; tuberculosis of all parts of the body except the meninges and brain, and several other chronic diseases. During the digestion of a meal rich in carbohydrates and in patients whose diet includes an excessive proportion of carbohydrate and hydrocarbon foods, the lymphocytes are relatively and absolutely increased. During starvaton the lymphocytes are relatively and sometimes absolutely increased as long as the glycogen and fats are being utilized as foods. During lysis in pneumonia and during convalescence in scarlet fever the hyaline cells are increased. After injury to the spleen or to any great area of lymphoid tissues the large hyaline cells are usually considerably increased. Relative or absolute lymphocytosis is usually present in scurvy, pernicious anemia, chlorosis, general debility, late typhoid hemophilia, exophthalmic goiter, and sometimes associated with malnutrition. In lymphatic leukemia the increase in hyaline cells may be tremendous. The small hyaline cells are most abundant in the less malignant and chronic lymphatic leukemia, the larger forms in the more malignant acute lymphatic leukemia and in the terminal stage of the chronic type. In the terminal stage of myeloid leukemia the hyaline cells may predominate and may seem to be exclusively present but in this case the hyaline cells are really of the myelocytoid type and are derived from bone marrow. The oxidase reaction may or may not be present in these hyaline myelocytes. (Plate XIII) In the presence of inflammation involving lymphoid
tissues the hyaline cells are increased and this increase is associated
with many structural changes in large and small lymphocytes and endothelial
cells. The small lymphocytes then show less distinct nuclear structures,
the nuclear limits are less well defined, there is less intensely basophilic
protoplasm, the protoplasm is more abundant, and basophilic granules appear
occasionally in the protoplasm. The large lymphocytes include some which
are smaller than normal, though still distinctly larger than the small
lymphocytes. These show less intensely basophilic protoplasm and occasional
basophilic granules.
The endothelial cells present nuclei larger than
normal, with less marked affinity for basic stains. The protoplasm presents
a swollen appearance and it flattens out on the warm slide very noticeably.
The cell outlines are indistinct and often ragged. Granules do not appear,
though sometimes there may be inclusions of fragments of other cells, of
bacteria or of foreign particles.
Lymphopenia is of much less common occurrence. During the digestion of fats and proteins, in some cases of tuberculosis and in some cases of lymphosarcoma the lymphocytes may be reduced to a few hundred in number per cubic millimeter of blood. They are relatively diminished in all conditions associated with marked neutrophilic leucocytosis but are often actually slightly increased in these diseases. Direct effects of vertebral lesions upon lymphoid tissue have not been observed, but indirectly very marked changes in lymphoid tissues may be due to such lesions. Space permits only a few references to these conditions. Lesions of the cervical and upper thoracic vertebrae affect the cirulation through the mucous membranes of the head and throat. A mild, chronic congestion of these tissues results. With this congestion, there is a moderate but persistent edema and some lessening of the alkalinity of the tissue juices. The lymph from tissues so affected passes into the lymph nodes, and these are stimulated into increasesd activity. The small normal lymphoid tissues of the nasopharyngeal region are often so affected and adenoid growths result. Moderate non-infectious enlargement of the tonsils is another such result of cervical or upper thoracic lesions. Enlargement of the cervical chain of lymph nodes results from longer existence of the same lesions. Immunity is diminished in all tissues affected by lesions as well as by the engorgement and hyperplasia of the lymphoid tissues. Infection of the tonsils is a later result of the lesions. Tubercular infection of the cervical lymph nodes is partly due to local lowering of the immunity of these glands and partly to systemic conditions, themselves often due to mid-thoracic lesions. The common infectious agents are almost universally present. Lesions of the ninth thoracic vertebra cause dilatation of the splenic blood vessels and decreased tone of the muscles of the splenic capsule. With the congestion thus produced there is inevitably some hyperplasia of the splenic lymphoid tissue. Lesions of the lower thoracic vertebrae cause mild chronic congestion and some loss of tonicity of the intestinal walls. With the resulting mild, chronic stasis, there is a mild but constant edema and a constant, mild poisoning due to the stasis. Hyperplasia of the lymph nodes of the intestinal tract is very common under such conditions. Lesions of the third lumbar and neighboring vertebrae cause mild and chronic congestion of the uterus. With this congestion there is edema and diminished alkalinity of the tissue juices. The weight of the edematous membranes increases with the persistent congestion though this may not be severe in degree at any one time. A serous polyp may result or an area of lymphoid tissue in the immediate vicinity of the edematous region may proliferate and form a lymphoid polyp of the cervix. In other cases there may be marked connective tissue proliferation and a fibrous polyp is produced The character of a polyp produced by upper lumbar lesions may pass through these three stages in order, in experimental animals, and a similar progression is quite possible in the human subject. In many areas of the body similar relations in pathogenesis
may be observed. Such relations are suspected when the blood cells include
immature or other abnormal forms of lymphocytes associated with a few granular
myelocytes and other evidences of disturbed circulation through the red
bone marrow of the bones concerned in the lesion.
A few other large hyaline cells may be found in very small numbers in normal adult human blood; these are found in considerable numbers under abnormal conditions. Turck cells are somewhat like ordinary large hyaline cells. The origin of Turck cells is not certainly known; they are increased under certain pathological conditions, and they are considered identical with plasma cells by several writers. Turck cells are hyaline cells with intensely basophilic protoplasm and deeply staining nucleus. The spongioplasm is usually distinctly visible and vacuoles are frequently present in the cytoplasm. Fatty material may be stored in vacuole-like areas, thus producing the foam cell type. The protoplasm presents a somewhat granular appearance but contains no real granules. These cells are ten to fifteen microns in diameter. They are ameboid and phagocytic, and often contain fragments of red cells. This is particularly true in those diseases associated with blood destruction, such as malaria. The nucleus is often eccentric and may be altogether free from a cytoplasmic covering upon one side. They are certainly concerned in the healing of wounds, and they seem to be derived from the adventitial cells. Plasma cells are like Turck cells except that they are often angular on account of pressure conditions; the nucleus is eccentrically placed, and very often the nucleus contains more definite chromatin masses which may show a wheel-like arrangement. The nucleus often lacks any recognizable protoplasmic covering for half or even more of its surface. The protoplasm is often vacuolated in the vicinity of the nucleus. The protoplasm is intensely basophilic at its periphery and very rarely can fine neutrophilic or basophilic granules be demonstrated in the region farthest from the nucleus. These cells are not found in normal blood. They may be abundant in inflammatory conditions and seem to be concerned in regeneration. They are derived from small lymphocytes, probably those of adjacent tissues. Myeloplaxes are very large hyaline cells which are
very rarely found in the circulating blood. They are identical with the
megakaryocytes of the red bone marrow.
Hyaline myelocytes are not found in normal blood. They are present in very large numbers in late stages of chronic or in rapid and severe acute leukemias. They may be found in small numbers when the bone marrow is invaded by malignant disease, especially in cancer metastases. They are then associated with other types of myelocytes and myeloblasts. Hyaline myelocytes have very large, spherical nuclei,
usually feebly staining, and a very narrow rim of protoplasm, usually with
very marked affinity for basic stains. No granules are found by the ordinary
staining methods. They vary in size, the smaller being distinguishable
with difficulty from small lymphocytes and the larger having a diameter
of forty microns or more. Every size between these may be found in severe
cases of either lymphatic or myeloid leukemia. (Plates XII, XIII)
The relations of the cells of the reticulo-endothelial system to the large phagocytic monocytes of the blood has been the subject of much study, yet many problems remain unsolved. That certain of the phagocytic monocytes found in the blood stream under abnormal circumstances are derived from the endothelium of the sinuses of the bone marrow, spleen and other lymphoid tissues, and probably from the liver and from certain glands of internal secretions is fairly well demonstrated by experimental and by pathological findings. Large, hyaline, mononuclear, phagocytic cells are found in the blood stream, a few normally, and many under abnormal conditions. Their presence in more than 1%, or in abnormal forms, indicates some definitely abnormal condition in the body. If they are merely increased in number but present no definitely abnormal forms, it may safely be concluded that there is some circulatory disturbance affecting the spleen and the liver. If they show vacuoles or inclusions, the significance depends upon the nature of these abnormalities. If they are immature and are derived from lymphoid tissue, it may be concluded that there is a chronic infectious process present in the body and that this affects a considerable area of lymphoid tissue. If many myelocytoid forms of granular cells or if a few immature red cells are present without other evidences of anemia, then there is some marked disturbance of the red bone marrow; if there is no evidence of serious disease of the red marrow the disturbance may be merely circulatory. If excessive numbers of the endothelial cells are present, with high red cell and rather high white cell counts, without other evidence of visceral disease, then it may safely be concluded that there is some very considerable area of the vascular bed in which the circulation is inefficient. Cardiac inefficiency is suspected in such conditions. The endothelial cells which normally remain within the lymphoid tissues are found in the circulating blood when there is any chronic inflammatory state which affects these tissues. These cells also may be found in the blood stream of an individual who suffers from the effects of ninth thoracic or neighboring lesions; in this case the cells are derived from splenic sinuses. The cells are often called splenocytes because they are so commonly derived from the spleen but they may be derived from any lymphoid tissues which have been affected by inflammatory conditions. They are not commonly derived from lymphoid tissues other than the spleen as a result of the direct effects of bony lesions, on account of the anatomical peculiarities of the tissues concerned. Large mononuclear phagocytes containing fragments of erythrocytes and particles of hemoglobin or of hemoglobin derivatives are found in the circulating blood under several quite different conditions. Such cells are often found in the blood after an attack of pneumonia, and are undoubtedly derived from the adventitial cells of the lungs. Occasionally such cells are found in the blood of persons with mitral lesions; in this case they are also from the pulmonary adventitial cells and they are a result of the excessive pulmonary congestion They may also be found, less frequently, in persons with bony lesions which affect the heart and thus the pulmonary circulation, or which interfere directly with the pulmonic vasomotor centers in the upper thoracic spinal centers. Endothelial cells containing fragments of erythrocytes or the brownish granules of one of the hemoglobin derivatives are usually present in the blood during an attack of malaria and for some time afterward. These same cells ingest and probably destroy the malarial plasmodium. The organism of histoplasma capsulata was found within endothelial cells and large lymphocytes in the blood of one of our patients, and the blood of inoculated guinea pigs contained many endothelial cells containing the organism. (Plates X, XI) During the course of pernicious anemia, the endothelial cells of the sinuses of the spleen, lymph nodes, bone marrow and hemolymph glands ingest great numbers of the abnormal red cells, and the endothelial cells found in the blood stream which contain fragments of red cells are probably derived from those areas. Whether the Kupffer cells commonly gain entrance into the blood stream is not known; that they do pass into the blood stream under experimental conditions seems definitely verified by Sabin and others. The Kupffer cells are abundantly filled with fragments of red blood cells during relapse in pernicious anemia, and this is true also of sickle-cell anemia and of other diseases characterized by abnormal fragility or abnormal structure of the red blood cells. Endothelial cells carrying granules of melanin are often found in the circulating blood when melanotic tumors are present anywhere in the body, and are more abundant when there are metastases in the liver, lungs, spleen or bone marrow. The amyloid substance is first found in the Kupffer cells of the liver when that gland undergoes amyloid degeneration. Endothelial cells containing granules of amyloid or a precursor of that substance are often found in the circulating blood under such circumstances. Endothelial cells often carry indophilic granules and such endothelial cells are rather abundant when there is an abnormal condition of the liver. When the neutrophiles as well as the endothelial cells of the blood carry indophilic granules some disturbance of sugar metabolism is suspected and a determination of the sugar tolerance curve is indicated. While patients with marked indophilia occasionally show no further evidence of disturbances in sugar metabolism, yet the relation is sufficiently common to warrant further investigation. The large phagocytic cells carrying iodophilic granules are also found when there is a marked disturbance in protein katabolism. Such conditions occur during the absorption of chronic pus foci, during the period of absorption after pneumonia, during the absorption of the products of degeneration of a tumor of any kind or of the absorption of any degenerating tissues of the body, or during rapid loss of weight after the fat has been absorbed during fasting, or even when a patient with intestinal atony is for some time on a heavy protein diet. The endothelial cells seem to have some especial affinity for fat, and droplets of fat are occasionally found in these cells in the blood stream. When there has been any injury to the shaft of a long bone, or when the fatty marrow has been invaded by infectious processes or by metastases of any malignant neoplasm, fatty globules are often found within the phagocytes of the circulating blood, including the endothelial cells. Fatty globules of small size may also be found free in the plasma under these conditions. Endothelial cells containing fatty globules are also found, occasionally, in disease or abnormal circulatory conditions affecting the liver, even though the hepatic disorder may not be very severe. When the fat of the body is undergoing rapid disintegration endothelial cells carrying fat are present; this is significant in patients who are reducing weight too rapidly. During the rapid absorption of pus, rapid degeneration of tumors, rapidly growing cancer, rapidly progressing pulmonary tuberculosis, and similar states these fatty inclusions within endothelial cells are occasionally found. When the cells are stained by ordinary methods the fatty globules appear as vacuoles. When stained by osmic acid or Sudan III their fatty nature is clearly shown. Metallic poisons are often stored in the endothelial cells and occasionally these cells are found in the blood stream. Mesotherium is so stored, and this may be one cause of obscure anemias. Lead particles also are so stored and these have been found in the circulating blood in cases of chronic lead poisoning. In an obscure case in our laboratory in which pernicious anemia was strongly suspected the finding of metallic particles in several large phagocytic monocytes in the blood smears led to the correct diagnosis of chronic lead poisoning. The endothelial cells of the peripheral blood are increased after emotional excitement, especially after fright and anger. Human beings who have undergone splenectomy do not show this reaction. From these and other related facts it may be concluded that during emotional states the contractions of the spleen force these cells out and into the blood stream. After removal of the spleen or of all or part of the sympathetic ganglia from the abdominal region the reaction does not occur in animals. Human subjects and animals with lesions of the ninth
thoracic vertebra (and, in less marked degree, neighboring vertebrae and
ribs) show higher than normal numbers of large hyaline cells in the peripheral
blood; no doubt this is due to the chronic slight congestion and the chronic
slight atony of the spleen due to the lesions.
A very brief review of the studies made of the reticulo-endothelial system may be useful. The discussions by Aschoff first aroused general interest in the subject. Very many histologists and pathologists have made reports; unfortunately the cells have received many names and many descriptions because the methods employed have produced so many reactions on the part of cells which were essentially, of the same class and of similar, if not identical, structure. The descriptions of the phagocytes of the blood and the tissues given by Metchnikoff are classical. In his reports the neutrophiles of the blood are called microphages and the larger cells of the tissues macrophages. The macrophages are phagocytic and are usually found lying free in the meshes of the connective tissues around the smaller blood vessels and the capillaries. Because they are especially abundant in that location they have been called adventitial cells. Because they were observed by Ranvier to present peculiar budding processes he called them clasmatocytes. With ordinary staining methods they are not distinguished from the fibroblasts of the connective tissues. The sinuses of the bone marrow, the spleen and other lymphoid tissues, the hemolymph glands and perhaps the tissue spaces of certain of the glands of internal secretions are lined with cells which resemble the endothelium of ordinary capillaries to some extent, but which are definitely phagocytic and which are able to store both particulate and colloidal dyes in such a manner as to prove them distinctly different from ordinary endothelium. The Kupffer cells of the liver, the podasteroids of the brain, the adventitial cells of nearly all the body, the plasma cells of the loose connective tissues and of the omentum as well as the cells of the sinuses of the bone marrow, spleen and other lymphoid tissues may, under certain physiological or pathological conditions be carried from many viscera in the blood stream. They may reach the blood by way of the lymph channels and the thoracic duct under certain circumstances. They can be cultivated in vitro and their development watched. There is very good reason for supposing that the words tissue macrophage, blood monocytes, clasmatocyte, fibroblast, hemohistioblast, wandering adventitial cell, endothelial cell and other terms less commonly employed are really different names for the same cell which presents somewhat different appearances under differing circumstances. These cells are capable of developing from one form into certain others according to the needs of the body at any given time. Their developmental potentialities are still a subject of considerable discussion and of intensive experimentation. The endothelial cells are important in the protection of the body against foreign substances and infections and they are concerned in the development of tubercles, together with the lymphocytes. In tuberculosis the blood often contains a marked increase of these cells. The blood of children with tuberculosis usually shows these cells abundantly. Further study of these cells should be made. With a definite understanding of their functions more adequate methods of diagnosis and therapy should become possible. |
{kind=link}