
|
The direct effects of bony lesions on blood cells are chiefly due to changes in the red bone marrow. Since the ribs include the largest area of red bone marrow in the body, lesions of the ribs and the thoracic vertebrae cause more marked changes in the development of the erythrocytes and the granular leucocytes than do lesions elsewhere in the body. Some review of the structural relations is necessary for adequate discussion of the relation of the lesions mentioned and the development of blood cells. The cells concerned in hematopoiesis are described in the chapters on the development of erythrocytes, neutrophiles and other granular leucocytes in this book. The innervation of the red bone marrow is of interest in this connection. The nutrient arteries, veins and nerves enter together at the nutrient foramina of the bones. The vaso-motor nerves are derived from the lateral chain of sympathetic ganglia, and the cells of these are controlled by the nerve centers in the lateral horn or homologous areas of the spinal cord. The segment from which the vaso-motor control of any given bone is governed is that segment most closely associated with the anlage of the bone during early embryonic development. Since there is considerable shifting of the embryonic skeletal structures and since the metameric nerve relations are maintained during the shifting the adult innervation of the bones presents many puzzling features. The problems are solved, however, by a study of the embryologic relations of bones, nerves and muscles. The vaso-motor nerves follow the blood vessels, chiefly the arteries and arterioles, to every ramification within the red bone marrow, and they terminate in nerve endings like those upon other blood vessels of the body. The endings are most abundant upon the arterioles, and are present less plentifully upon the venules, arteries, veins and capillaries in order. Another group of nerves terminates in fine, brush-like endings which branch freely among the hematopoietic cells of the red marrow. All these nerves are nonmedullated. Medullated nerves are afferent, and are derived from
the posterior root ganglia of the spinal segments from which the efferent
nerves arise. The central prolongations of the cells of these ganglia enter
the spinal cord and are distributed to the gray matter of the posterior
horn and the lateral horn, where this is present. Throughout the thoracic
spinal cord the costal nerves are of especial interest since they innervate
the areas of bone marrow of the ribs, the most important hematopoietic
tissues of the body. The sensory nerves from the red bone marrow are not
intimately connected with the brain centers, and very serious disease of
bone marrow may be present without causing discomfort. After the disease
has extended into the periosteum there is usually some dull pain in the
affected bone. The functions of these sensory nerves are not well understood
but it is certain that they are associated with the local vaso-motor centers
and that the impulses carried into these centers from the bone marrow modify
the circulation through all the tissues controlled by those centers.
Lesions affect the functional relations of the hematopoietic tissues in much the same manner as that noted in the relations of bony lesions with the viscera generally. A lesion of a vertebra or a rib is a disturbed relationship of that tone with its fellows of such a nature that a persistent strain is produced without causing any actual rupture of ligaments. The position which the bones assume is that which may be normal under some circumstances; for example, the vertebrae have one relation with one another when the spinal column is flexed and another relationship when the spinal column is erect. If any two vertebrae maintain the relations normal to the flexed spinal column when the column has returned to its erect position, those two vertebrae are not in normal relations; this is a vertebral lesion. Ribs are approximated when the body is bent to one side; if any rib maintains that same position when the body returns to the erect position, that rib is lesioned. In either case there is a persistent strain upon the articular surfaces and the ligaments are subject to abnormal tension on one side, and to abnormal loosening on the other side of the joint. When such a lesion is present the surrounding tissues become edematous; the tissue fluids become less alkaline than normal and there is a slight but persistent local congestion with some retention of the waste products of katabolism and some lack of normal oxidation processes of the cells of the immediate vicinity of the lesion. These changes are always present when a costal or
vertebral lesion has been present for a few days and they remain present
as long as the lesion remains
The sympathetic ganglia which lie near the costo-vertebral articulations are subject to these same pathogenic influences. The non-medullated nerves leaving the sympathetic ganglia are somewhat more seriously affected than are the medullated nerve fibers, because the medullary sheaths of the latter protect the nerve fibers in some degree from pressure and from the tissue juices. The nerve fibers which enter the nutrient foramina of the bones, to be distributed to the blood vessels and to the hematopoietic cells of the red bone marrow, are subject to the effects produced by both the pressure of the edematous tissues and the abnormal chemical composition of the tissue fluids around the lesion. When the lesion is limited to one or two spinal segments the area of bone marrow affected may be small and only a few abnormal blood cells be produced. When lesions involve several segments or when the ribs fail to move properly in respiratory activity the blood contains many abnormal cells. The anemia thus produced may be slight or it may be profound, according to the manner in which other areas of red bone marrow in the flat bones, the small bones and the ends of the long bones compensate or fail to compensate for the costal hematopoietic deficiencies. Any lesion of any bone in the body affects the circulation and the innervation of the red bone marrow of that bone and usually of one or two adjacent bones. A few abnormal blood cells are the result of such an abnormal state of the local red marrow, and it is possible to find abnormal cells in the blood of an individual with such lesions provided the blood smears are carefully studied. When the abnormal area of red bone marrow is very small the abnormal cells are few. The bone marrow of the ribs of human subjects is
subject to certain disturbances due to the habit of mankind.
It must be remembered that the nutrient blood vessels and nerves lie in a groove along the lower edge of each rib and that the largest nutrient foramen is near the angle of the rib. Animals walking on four legs have the ribs hanging downward from the spinal column, and as the animal walks or runs the spinal column and the ribs are moved back and forth gently; the intercostal tissues are constantly relaxed and there is rarely any abnormal pressure upon the nutrient vessels and nerves. Mankind walks on two legs and the spinal column is held more or less erectly. The ribs may be allowed to droop, in which case the intercostal tissues are subjected to some slight but persistent pressure. The thorax may be held erect, by means of muscular activity along the spinal column, in which case also the intercostals tissues are subjected to some pressure. If the respiratory movements are normal alternate relaxation and contraction of the intercostal muscles secures fairly normal innervation and circulation of the red marrow of the ribs. But if the respiratory movements are impeded, so also is the circulation of the rib marrow. Persons suffering from certain functional neuroses show abnormal thoracic rigidity with resultant anemia. The thoracic rigidity due to the neurosis or psychosis is very much like a lesion in its effects on the development of the blood cells. The tension of the intercostal tissues and the lack of respiratory movements leads to inefficient circulation and innervation of the red marrow with later development of typical costal anemia. In these persons there are other pathogenic factors which increase the anemia indirectly. The rigid thorax fails to give the heart the normal stimulation due to variations in the intrathoracic pressure; a weakened heart muscle and low blood pressure are common results. The venous return to the heart is also impeded by the lack of the normal variations in intrathoracic pressure. Inefficient diaphragmatic respiratory movements prevent the stimulation of the liver, the spleen and the pancreas due to the normal alternate contraction and relaxation of the diaphragm. Cholemia and increased rapidity of red cell destruction is a result of the abnormal hepatic condition thus caused. Toxemia and malnutrition are increased by the effects produced upon the stomach, spleen and pancreas by the diaphragmatic immobility and the blood cells are thus indirectly effected. The conditions responsible for the functional neurosis
may add other pathogenic factors to the anemia or not, but the respiratory
inefficiency due to the neurosis itself must be considered an important
factor in the anemia always present in these patients.
Certain local lesions exercise indirect effects upon the development of blood cells. Lesions of the tenth thoracic vertebra and of the tenth ribs affect the circulation of the blood through the liver and cause a slight but constant decrease in the tonicity of the muscular walls of the bile ducts. Lesions of the eighth, ninth and eleventh thoracic vertebrae and the corresponding ribs exercise a similar but somewhat variable influence upon the same tissues. As a result of the slight congestion and the slight edema always associated with these lesions together with the slight accumulation within the bile ducts, the bile passes into the venous blood and the lymph and thus into the general circulation. Bile pigments are slightly destructive to the blood cells, both red and white, and the bile salts are definitely destructive. Bile pigments may be recognized with sufficient accuracy for clinical purposes by the Gmelin test of the scrum. Chemical tests for bile salts are difficult to make without using too great an amount of the blood, but their presence may be suspected when the surface tension of the blood plasma or the blood serum is lowered, and when bile pigments are known to be present. In such cases the erythrocytes are fragile and blood shadows may be found in the smears and on the warm stage. The protoplasm of the neutrophiles and the hyaline cells show frayed and irregular outlines. The eosinophiles do not show this effect. The nuclei are not so seriously affected and naked nuclei or masses of nuclear material without recognizable protoplasm are abundant in the blood smears. The small basophilic or amphophilic cells, often called mast cells, are found in normal adult human blood in very small numbers; often none can be found in a differential count of five thousand cells or more, or one or two might be found in a count of five hundred cells. These are increased in certain forms of leukemia and other pathological conditions. They are also slightly increased as a result of any abnormal condition affecting the thyroid gland. Bony lesions of the first or second thoracic vertebra
and of the third cervical vertebra affect the circulation through the thyroid
gland, cause an edema and diminished alkalinity of the tissue fluids of
the gland, and increase the mast cells in the blood. These lesions and,
occasionally, lesions of adjacent vertebrae, usually tend to increase basal
metabolism, though hypothyroidism occasionally follows later. When mast
cells are present in increased numbers or when only a few are present but
these present evidences of immaturity of structure, a determination of
the basal metabolism of the patient is indicated. Correction of the lesions
found on examination is followed by return of the basal metabolism to normal
and by the disappearance of the excess of mast cells, if the thyroid pathology
has not progressed to tissue destruction of considerable extent.
The hyaline cells show the effects of bony lesions by way of the changes due to the circulation through the spleen, so far as the lymphocytes are concerned, and by way of circulatory disturbances elsewhere in the body so far as the less common forms of hyaline cells are concerned. Bony lesions affecting the spleen include the ninth
thoracic vertebra and the ninth ribs, especially. The seventh, eighth and
tenth thoracic vertebrae and the eighth and tenth ribs, especially on the
left side, also affect the splenic circulation. When such lesions are present
the blood smears show an increase in the number of large hyaline cells
and of splenocytes. The large lymphocytes and the splenocytes are derived
from lymphoid trabecular and pulp. When such cells are found abundantly
in the blood smears, with no evidence of leukemia or other gross pathology
of the hematopoietic tissues, some abnormal circulatory condition of the
spleen or of some other large area of lymphoid tissue is strongly suspected.
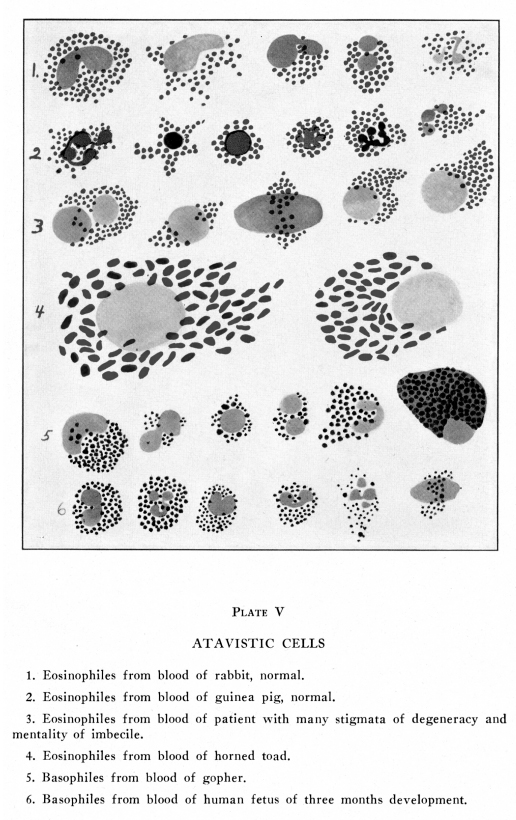
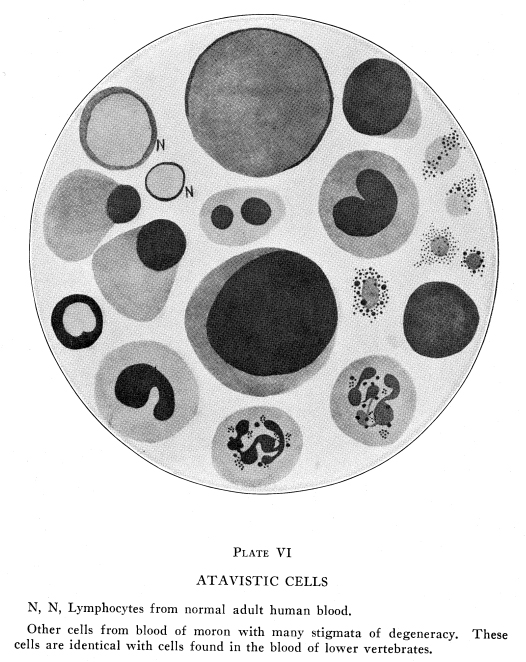
Eosinophiles of myelocytoid or immature structure are found in the blood stream whenever there is marked congestion of the ovaries or the testes. After sexual excitement such cells are normally present in the circulating blood; they disappear within twenty to forty hours. They appear in the blood of women at about the menstrual period. During adolescence and the climacteric they occasionally appear in the blood of either sex without evidence of any abnormal condition. When there is any abnormal congestion of either testis or ovary these blood cells are found and they may be of importance in diagnosis. Lesions of the eleventh thoracic or of the second lumbar vertebra cause a slight but persistent congestion of the reproductive glands. Myelocytoid eosinophiles are usually fairly abundant in the circulating blood under such circumstances. Correction of the lesion permits return to normal circulation and function of these glands, provided there has been no actual tissue destruction, and within a few weeks the peculiar eosinophiles are no longer found in the blood except under the physiological conditions mentioned above. (Plates V, VI) Secondary anemias due to malnutrition are often due
to bony lesions. Lesions of the fifth thoracic vertebra are especially
associated with occasional hyperchlorhydria and a tendency to gastric ulcers;
the anemia due to these conditions may be very severe. Lesions of the seventh
and eighth thoracic vertebrae and the associated ribs are commonly associated
with gastric atony, gastroptosis, and hypochlorhydria; the anemia due to
these conditions is not usually so profound as that due to fifth thoracic
lesions.
Lesions of the eleventh and twelfth thoracic vertebrae (and of the thirteenth and fourteenth thoracic, in animals) cause marked disturbance in the circulation and the secretion of the kidneys. The mild but persistent nephropathy thus produced causes a slowly developing secondary anemia which is very intractable until the lesion has been corrected. If the lesion has been present for more than a year, in laboratory animals, there is produced a permanent nephropathy. In human subjects the correction of the lesion within a few years after it has been produced results in an apparently complete recovery. It must be remembered that the human renal equipment is much greater than is necessary under normal and mildly abnormal circumstances. Any considerable amount of renal tissue capable of normal functioning is able to meet all ordinary and even quite heavy unusual demands upon the kidneys. Bony lesions cause anemia directly, by affecting the circulation and innervation of the red bone marrow, and thus preventing normal blood cellregeneration. Bony lesions cause anemia indirectly, by causing toxemia with resultant excessive blood cell destruction. Bony lesions cause anemia indirectly also by interfering with normal nutrition and preventing normal blood cell regeneration. |
{kind=link}
{kind=link}