
|
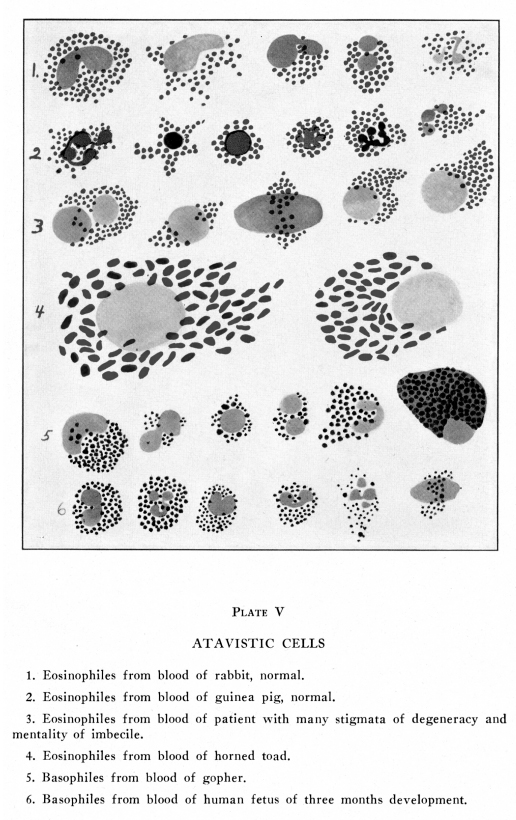
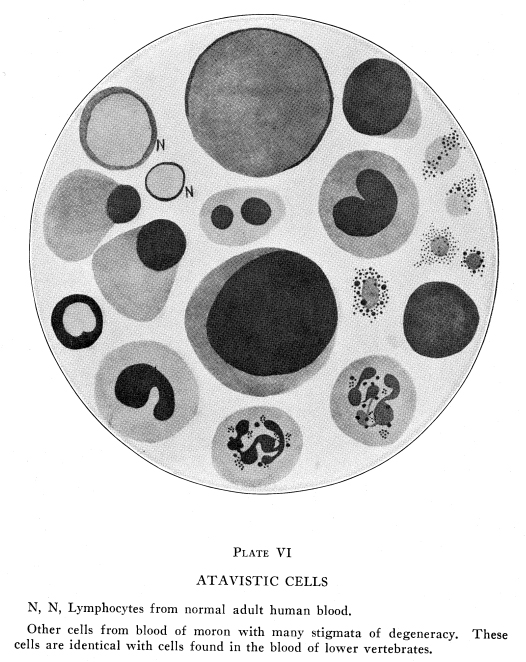
The cells of normal adult human blood include few forms, easily classified and with few or no intermediate types. Immature and abnormal specimens of blood present a great many forms of blood cells often classified only with difficulty and including many atypical and intermediate forms. Normal adult human blood cells include two chief groups, hyaline and granular. The hyaline cells all have hyaline basophilic protoplasm in which no granules are found by the usual methods of preparation, while the protoplasm of the granular cells contains granules which present typical characteristics in size and in staining reactions. Hyaline cells are further divided into lymphocytes, which make up the largest number of these cells, and monocytes. In embryonic and abnormal blood there are also endothelial cells and myelocytes which have hyaline basophilic protoplasm. The lymphocytes are further divided into small, medium and large. Extremely large hyaline cells and atypical forms are found frequently in the blood of lower animals, in embryonic human blood, and in adult human blood under abnormal conditions associated with other reversionary traits. Granular cells are divided according to the nature of the granules into neutrophiles, in which the granules are small, abundant and feebly eosinophilic or neutrophilic; eosinophiles, in which the granules are larger and are intensely eosinophilic, and the rather scanty basophiles, in which the granules are large and are intensely basophilic. Amphophiles, in which the granules are large and may take eosin or basophilic dyes according to the concentration or reaction of the staining solutions, or can be so stained as to show eosinophilic and basophilic granules in a single cell, are extremely rare in normal adult human blood. They are often found in the blood of lower mammals, in embryonic human blood, and in adult human blood under certain abnormal conditions. (Plates III, V, VI) The lymphocytes of the blood are formed in the lymphoid
tissues of the body; there are a few which arise from other areas. The
granular cells are formed, during normal adult life, in the red bone marrow.
During embryonic and fetal life and under certain abnormal conditions the
white cells may be formed in other areas of the body including the spleen,
hemolymph glands, and in other viscera, and even in the fatty tissues of
the mesentery and omentum. The extent to which this process of leucocytopoiesis
may occur in the various organs of the body has been the subject of much
discussion. Under those conditions in which such extramedullary blood formation
occurs, there is a great amount of infiltration of the various tissues
with white cells. Cells undergoing dividion in the circulating blood are
fairly common under the same circumstances. It is quite possible that in
such cases leucocytopoiesis occurs wherever and perhaps whenever the cells
are permitted to find rest and food, and that accumulations of such cells
result whenever they are not speedily swept away. In vertebrates below
mammals and in certain of the lower mammals the leucocytes are formed in
extramedullary tissues throughout life.
The functions of the leucocytes include many activities. By virtue of their powers of ameboid movement and phagocytosis they are concerned in the absorption of fats and probably of protein and sugars from the intestinal tract. They serve as reserves for proteins and carbohydrates in the body. They ingest foreign particles and render them harmless to a surprising degree. They neutralize toxic substances whether these are produced by the cellular activities of the body itself, are produced within the body by parasites, are taken into the body with food or injected as therapeutic measures. They are not always able to do this perfectly, as is easily apparent, but their efficiency is surprising in many instances. They ingest small particles of foreign materials, bacteria, micro-organisms of several kinds, and the cells derived from malignant neoplasms and from diseased tissues. It is not possible to say to what extent life may be preserved by these activities. When any disease associated with profuse drainage
of pus is present, the number of leucocytes lost in a day may be more than
the number present in the total blood stream at any one time. Yet this
rapid formation and loss does not seem to exert any very serious drain
upon the blood forming tissues; these must, therefore, be fitted to produce
daily a number not very far below the total number in the circulation at
any one time, normally or abnormally. The dissolution of these white cells
must add considerably to the protein content of the blood, and there is
good reason to suppose that this elaboration of the nitrogenous elements
of the food is one of the functions of the white cells. No doubt the storage
of these protein substances within living cells, thus maintaining a normal
level of the soluble proteins of the blood, is a very important function
of the cells.
It is possible to determine with a fair degree of accuracy whether the cells arise from bone marrow or not, by the use of the oxidase reaction. This test is rarely of value in diagnosis but it has given some interesting information about blood cells. Smears stained with alpha-naphthol and dimethylparaphenylene-diamine show this reaction. By means of an oxidizing ferment, present in all cells, this stain produces indophenol blue. This reaction is not given by cells derived from lymphoid tissue, even that which is located within the bone marrow. Hence the reaction has a certain value in determining the origin of non-granular cells and of atypical granular cells under certain conditions. The granular basophilic cells (mast cells derived from the tissues) also fail to give this reaction. Large hyaline cells with large nuclei, sometimes showing karyokenesis, may be found under any circumstances associated with increased activity of the blood-forming organs. They may give the oxidase reaction by which they can be distinguished from the large hyaline cells of the splenic pulp and inflamed lymphoid tissue. Immature hyaline myelocytes do not give the oxidase reaction. Large hyaline cells, with protoplasm showing some affinity for acid stains, not giving the oxidase reaction, may be found in the blood of pregnant women, at about the fifth month especially. These are probably derived from the placenta. Tumor cells may occasionally appear in the blood.
They are rarely so large as the large hyaline cells, though they may be
even larger. They have deeply staining nuclei, usually round, sometimes
showing abnormal karyokinetic figures. Their protoplasm is acidophilic.
They do not give the oxidase reaction. They cannot be considered of marked
significance unless they are present in considerable numbers, show abnormal
karyokinetic figures, and are associated with other symptoms characteistic
of tumor.
Normal adult human blood contains a variable number of leucocytes, generally between 5,000 and 8,000 per cubic millimeter of peripheral blood. The small lymphocytes are the smallest of these, and the large mononuclear hyaline cells the largest. The neutrophiles are most abundant. In the climate of Los Angeles we find average normal counts of 7,500, varying from 4,800 to 9,500 in persons apparently in excellent health. Neutrophiles . . . . . .
. . . . 60% to 70% 3,000 per cu.mm.
The total leucocyte count, the differential count and the actual numbers of the various cell groups vary almost continually both in normal and in abnormal persons. The granulocytes seem to be thrown into the circulation, normally, in showers. The utilization and destruction of these cells progresses fairly steadily. Either the formation or the destruction of these cells can be hastened or diminished by various normal physiological conditions. In disease many factors may be active which increase, diminish or modify these physiological factors. Increased formation or increased destruction may be due to the action of factors not present in health, or, at least, not concerned in blood formation and blood destruction in health. The manner in which the white cells are thrown into
the general circulation varies greatly for different persons. In one family
studied in our laboratories the showers of neutrophiles appeared at intervals
of about two weeks. The period during which the heaviest shower of leucocytes
was passing into the peripheral blood was a time of physical and psychological
depression, not marked but definitely recognizable. In this family the
hyaline cells remained constant, varying only slightly from time to time,
as in other people.
Daily variations have been determined by several workers. Two high tides have been described, one occurring in the early afternoon, the other soon after midnight. There is some difference of opinion as to the exact hour at which the tide is highest. Rises of 1,000 to 2,500 cells have been reported for this tide. The tides occur with reasonable promptness no matter whether food, rest, exercise, sleep and other physiological conditions remain regular or whether these habits are subjected to considerable modification. A low blood pressure has been reported for these same hours. The afternoon tide should be taken into consideration when blood counts are made for the sake of diagnosis at that time of the day. The rise which occurs after midnight is less important because it is only in emergencies that counts are made at that hour. In emergencies differences of 2,000 white cells are not apt to be important. Still, the fact that a high tide of white cells does occur at that time of the night should be kept in mind. For accurate work the cell counts should always be made at the same time of the day for each patient, and, as nearly as is practicable, during the early afternoon hours for all chronic patients. The distribution of the white cells within the peripheral
blood of different parts of the body may be changed considerably by varying
the vasomotor control of the blood vessels. For this reason it is necessary
to be very careful to avoid irritation of the skin when preparing to take
the blood for a count. The use of rubbing to redden the skin in order to
secure blood more easily, or of irritating , heating or chilling solutions
for the sterilization of the skin may cause a variation of 2,000 or more
cells per cubic millimeter of blood. Vasoconstriction of a part causes
diminished white cell count; vasodilatation of a part causes increased
cell count.
The term leucocytosis applies to a temporary and marked increase in the leucocyte count, and it is commonly used with respect to the neutrophiles only. Increase in the lymphoid elements is called lymphocytosis or lymphemia and increase in the eosinophiles is called eocinophilia. General or neutrophilic leucocytosis, lymphocytosis or eosinophilia may be caused by physiological or pathological states. The physiological causes of neucocytosis should be thoroughly understood in order that pathological variations may be properly interpreted. Increase in the number of any one cell type usually is associated with at least a slight rise in other cells, though this is not invariably the case. Marked increase in any one group of cells naturally diminishes the percentages of other cell groups. For this reason it is not wise to draw conclusions from a differential count alone. Active leucocytosis (Ehrlich) is an increase in the neutrophiles or phagocytic cells, ameboid cells which respond to chemotaxis. Passive leucocytosis (Ehrlich) is an increase in hyaline cells, supposed to be passively washed out of lymphoid tissue. These terms are not now in general use. The hyaline cells are often ameboid and emigration of these does occur. Mixed leucocytosis is a term which has been used in different ways. It is now used to indicate leucocytosis in which many myelocytes are present. The condition is most marked in young children. In any severe or prolonged leucocytosis myelocytes usually appear, especially after severe hemorrhages. Pseudoleucocytosis (Emerson) is a term applied to certain changes in white cells not associated with increase in blood count but which have the same significance as true leucocytosis. These include indophilia, degenerations of leucocytes, increase in the relative number of neutrophiles, presence of myelocytes and other immature forms, fragmentation of nuclei, fragmentation and erosion of protoplasm and irregularities of staining. Increase in the total leucocyte count without variations
in the percentages of cell types occurs under several physiological conditions.
Dilatation of the capillaries (as, for example, by too great rubbing in
an effort to clean the skin before making the prick to secure blood) increases
the total leucocyte count without causing any recognizable or constant
change in the cell relations. The leucocytoses associated with digestion,
pregnancy, cold bathing and massage are of this general type.
Digestion leucocytosis occurs after a meal heavy in protein food, taken after a short fast or after a few days of vegetarian food. This form of leucocytosis does not appear in vegetarians, nor after a meal of low protein content; it does not appear in any case in a person habitually on high protein diet. It is often noted in diabetics. It does not appear in gramnivorous animals. It occurs markedly in babies placed on cows milk for the first time. Persons suffering from habitual constipation do not usually show this digestion leucocytosis. Digestion leucocytosis fails to occur if the gastric juice contains very little or no free hydrochloric acid, in which case the digestion and absorption of protein foods are delayed. From all these facts it has been supposed that digestion leucocytosis is a reaction to the foreign protein absorbed from the intestinal tract. The leucocytosis thus caused is often general in type, but a moderate neutrophilia is fairly common. This leucocytosis appears within the first hour, increases for two to four hours, sometimes to one and one-third the normal count, then gradually diminishes until the normal count is regained, about six hours after the test meal. Individuals who are constantly over-fed with an abundance
of protein foods usually show a total leucocyte count about 10,000 per
cubic millimeter in this climate.
The first day or two days of fasting or starvation is associated with a moderate rise in the leucocyte count, chiefly due to increase in the neutrophiles. After the second or third day the neutrophiles fall rapidly for a day or two, then slowly for as long as the fast is maintained. The hyaline cells fall slowly and steadily after the second or third day. The eosinophiles are relatively increased but not absolutely affected during the first week or so. During the absorption of muscle, in a long fast, the eosinophiles are absolutely as well as relatively increased. Pregnancy is usually associated with a mild leucocytosis, especially in primiparae. In our records of women who had had several counts during girlhood, before marriage, after marriage, before pregnancy and during pregnancy, a slight increase in the total count was observed before menstruation and soon after the beginning of pregnancy. This leucocytosis has usually been general in type in normal cases, but in a few apparently normal cases and in most cases with mild complications the increase in cell count has been mostly due to increase in the neutrophiles. Moderate eosinophilia usually preceded menstruation and may be rather marked during pregnancy, especially at about the third and fourth months. At these times some congestion of the ovaries is probably present. Leucocytosis of normal pregnancy rarely exceeds 15,000 cells per cubic millimeter and usually remains below 12,000. Abnormal conditions often cause variations which are more marked than would be expected in non-pregnant women under the same circumstances. Leucocytosis increases during labor, sometimes very
considerably, and diminishes rapidly so that in uncomplicated cases within
two weeks or less the leucocyte count is about normal. During involution
there may be quite a marked increase in endothelial cells.
Very heavy work causes leucocytosis. After strenuous exercise with almost complete exhaustion counts of 14,000 to 25,000 leucocytes have been reported. The neutrophiles are more greatly increased than are other cells, though absolute eosinophilia is always present in some degree. Increase in the lipase of the circulating blood, most abundant in the lymphocytes, has been reported during fatigue. The leucocytes are increased by traveling to high altitudes, at the rate, approximately, of 1,000 cells for each 1,000 feet of elevation. The large mononuclears are more rapidly increased than are the neutrophiles. The count returns to normal within about ten days if the subject remains at the high altitude. If he descends within a few days the leucocyte count drops to normal within about ten days. The person who lives at a high altitude, then descends to sea level shows a drop of about 1,000 cells for each 2,000 feet, and the count returns to normal within four or five days, if he remains at the low altitude. The leucocytopoietic tissues accommodate their activities to the demands of the individual without regard to altitude. Leucocytosis due to the agonal state is now supposed
to be of rare occurrence. Conditions which cause death are often associated
with leucocytosis. With slowing of the circulation there is an accumulation
of the white cells in the peripheral vessels.
Leucocytosis, usually mild in degree, follows tissue injury whether or not hemorrhage occurs. Post-hemorrhagic leucocytosis varies considerably, and bears no relation to the extent of the hemorrhage. Mild leucocytosis may be present after either severe or moderate hemorrhages, and marked leucocytosis, even to 20,000 or more, may be present after moderate or severe hemorrhages. This leucocytosis has been supposed to be due to a flow of tissue juices into the vessels, in which case there should be a lymphocytosis. Probably the flow of tissue juices into the vessels is associated with even more marked flow of the marrow cells into the circulation, in which case neutrophilic leucocytosis would, and actually does occur. Hemorrhages into the serous cavities (dural, peritoneal, pleural) cause leucocytosis amounting to two or three times the leucocyte count already present. This increase in leucocyte count begins almost immediately after the hemorrhage and continues more and more slowly for eight to twelve hours, when the numbers begin, at first very slowly, to recede. The normal number is reached during the succeeding three to five days, in uncomplicated cases. In doubtful cases two or three successive blood counts made during the six hours following the suspected hemorrhage indicate the leucocyte curve and may verify or eliminate the diagnosis of hemorrhage. Post-operataive leucocytosis commonly varies according to the amount of tissue injury sustained and may reach 20,000 or more. This leucocytosis bears no relation to the fever curve and it disappears within a day or a day and a half. Changing the packing on a wound also causes leucocytosis, mild and transitory unless there is considerable irritation of the tissues. This leucocytosis must not be confused with infectious leucocytosis. Post-operative leucocytosis disappears at about the time an infectious leucocytosis begins, and the infectious leucocytosis is almost always associated with fever and with other indications of infection. Chloroform often causes transient and usually mild
leucocytosis, but ether causes leucopenia more frequently.
Most acute pyogenic infections or febrile diseases cause leucocytosis. Low or absent leucocytosis may mean either very mild infection or very low resistance on the part of the individual. Diseases vary in their quality of arousing leucocytosis, as in their quality of arousing fever. In other words, the hematopoietic tissues react differently to different infectious agents and to different etiological factors. Leucocytosis depends upon the amount of toxin absorbed, as a rule; with drainage of an abscess the count drops quickly I uncomplicated cases Formation of exudates rich in pus cells is associated with higher counts than formation of non-cellular exudates, generally. The height of the count alone bears no certain relation to the severity of the infection. A small boil may cause marked leucocytosis if the infectious agent is of marked malignance and if the reaction of the patient is good. In one of our records a moderately acute exacerbation of a chronic appendicitis caused a rise of the leucocyte count from 11,000 to 32,000 cells within three hours. In another case of appendicitis with gangrene the count diminished from 25,000 to 3,000 cells within two days; death occurred two days later. Leucocytosis follows infection or other states usually causing leucocytosis only when the leuocytopoietic tissues are able to react to the demands made upon them. When the insult is too profound, or when the tissues are for any reason unable to react efficiently, then adequate leucocytosis does not occur. It is evident that in such conditions the prognosis is more gloomy for that reason. That the absence of leucocytosis is due to inadequate reaction and not to the mildness of the infection is suspected when there is iodophilia, increased nuclear average, fragmentation of the neutrophile nuclei with many nuclear pseudopodia, relative or absolute neutropenia, and the presence of many myelocytoid and endothelial cells in the blood. It should be noted that the conditions mentioned
as affecting leucocytosis also affect the temperature reactions to infection.
In the following conditions leucocytosis parallels the temperature curve;
pyrogenic infections generally, erysipelas, empyema, renal abscesses, pulmonary
abscess, acute bronchitis, pneumonia.
Leucocytosis is not always present but usually develops at some time during the course of the following diseases: small-pox, typhus, rabies, endocarditis, pleurisy, gonorrheal arthritis, renal colic, gout, bronchiectasis and certain cases of influenza. These various conditions, not primarily infectious, usually show marked leucocytosis with atypical characteristics. Metastases from malignant neoplasms may invade the peritoneum, pleura or red bone marrow. In the last case the blood picture may resemble that found in the leukemias or may resemble that of pernicious anemia. Malignant neoplasms occasionally cause neutrophilic leucocytosis, more often lymphocytosis, and this usually disappears after remove of the tumor. Lymphocytosis, rarely neutrophilic leucocytosis, often follows treatment of cancer by radium. Leucopenia often follows this treatment, and usually follows treatment by X-rays. Ovarian cyst with torsion of the pedicle causes marked leucocytosis; this may be of diagnostic value. The myxedema which sometimes follows thyroid operations (less commonly nowadays) may be associated with leucocytosis reaching 50,000 or more. Leucocytes are increased in patients with gastric hypersecretion, and diminished in patients with hypochlorhydria. Leucopenia is associated with achylia and leucocytosis with hyperchlorhydria, even in fasting subjects. Acute intestinal obstruction causes leucocytosis, usually of the neutrophilic type in adults. Lymphocytosis occurs frequently in children with obstruction. This should not be above 20,000 in uncomplicated cases. If the neutrophiles are relatively increased on the second or third day, or if the count continues to rise, infection and gangrene are suspected. Drugs used in the treatment of disease or inhaled or absorbed as an occupational condition may cause leucocytosis. Camphor is especially active in this connection. Leucocytosis follows administration of epinephridine hydrochloride. Immediately after injection all white cells rise, then the lymphocytes increase more rapidly, later the neutrophiles increase more rapidly. The reaction is due to the spasm of arterioles, venules and splenic capsule due to the drug. Other drugs cause leucopenia; the most common of
these are the coal-tar derivatives, lead, mercury, benzol, the chlorates
generally, and arsenic. Counts below 1,000 are not rare in patients who
have been treated with these, or with certain other less common drugs,
or whose occupation causes such drugs to be absorbed or ingested with food.
The term leucopenia is applied, usually, to counts below 4,000 cells per cubic millimeter of blood. Leucopenia is characteristic of many cases of influenza; is present in typhoid fever after an initial leucocytosis; in peritonitis during the rapid formation of purulent exudates; in tuberculosis of the lymph glands and in miliary tuberculosis, and in pernicious and aplastic anemia. Leucopenia is also present in many cases of severe pyrogenic infections to which the hematopoietic tissues are unable to react efficiently. Such cases are extremely serious. Agranulocytic angina is a peculiar disease characterized by extremely severe infection of the throat and sometimes of other mucous membranes, in which the neutrophiles almost disappear from the peripheral blood. The hyaline cells which are increased at the same time seem completely unable to meet the emergency and the condition is almost inevitably fatal. Radiation treatments given for leukemia, Hodgkins
disease and other abnormal conditions may reduce the number of white cells
to a dangerously low level, even to less than 500 cells per cubic millimeter
of blood. Since the neutrophiles are so important in immunity their reduction
may have serious results. Deaths from pneumonia during the course of radiation
treatment for leukemia are not infrequent. Careful use of radiation therapy
should prevent extremely low leucopenia.
Granules which stain with iodine and which may be either glycogen or some other substance, as peptone or amyloid-precursers, are sometimes found in the leucocytes and in the plasma. Normal blood contains, sometimes, a few of these iodophilic granules, but they are rare. They occur most frequently in the polymorphonuclear neutrophiles, but may be found in any of the leucocytes, possibly in the platelets, and occasionally they lie free in the plasma. Blood smears from a three-months fetus show iodophilic granules in the erythrocytes but not in the leucocytes. They are rarely present in the nucleated red cells, and, when present, they are round, very scanty, and lie near the nucleus. In the normoblasts of this fetal blood in which the nucleus is undergoing solution several rod-shaped iodophilic masses lie near the nuclear remnants. In erythrocytes which have lost their nuclei rod-shaped and round iodophilic granules may lie anywhere in the protoplasm. The chief diagnostic significance of iodophilic granules is their presence in considerable numbers in septic conditions, especially when the process is well developed. They are not found in the earlier stages of infection. Iodophilia is found in the following diseases: Abscesses, septicemia, empyema, pneumonia, septic peritonitis, pyonephrosis, tonsillitis, gonorrheal arthritis, gonorrheal or streptococcal salpingitis, purulent conditions anywhere in the body; and in gangrene, especially that of hernia or intestinal obstruction. They have been reported also for pernicious anemia, myelogenous leukemia, ovarian cyst with torsion of pedicle (in which case there is leucocytosis but not infection), and in cerebral abscess. They are not present in cerebral tumor, nor in diphtheria or tuberculosis unless secondary pyogenic infection occurs. They are absent in early typhoid but may be present after the second or third week. They are present in cases in which there is absorption of degenerating nitrogenous substances within the body, and they may be of use in differentiating abscess and benign tumor; or syphilitic from other forms of secondary anemia; or in the recognition of obscure pyogenic foci. After drainage of the pus or resolution in pneumonia the granules disappear very rapidly. Probably normal leucocytes contain glycogen in transient and varying amounts, according to the sugar requirements of the body. Under the abnormal conditions mentioned, however, the granules become more stable and are easily found in the blood smears. Normal blood stains a diffuse, pale yellow with iodine. The nuclei are lighter in tint. Rarely iodophilic granules are found in the plasma or platelets of normal blood. A positive reaction is shown by deep, or platelets of normal blood. A positive reaction is shown by deep, diffuse brownish color in many of the leucocytes, and by a recognizable number of brownish granules in the leucocytes, platelets and plasma. Endothelial cells in the blood and fixed cells of
the reticulo-endothelial system contain glycogen or some related substance
in granules and also in a more diffuse form. There is no apparent relation
between the degree of iodophilia or the number of iodophilic cells and
the amount of sugar in the blood.
These cells have received various names,--smudged cells, basket cells, fractured or fragmented cells. In smears which are carelessly made, many of the cells are injured; they may be spread out and smeared over the slide, or may be broken into fragments varying in size. They are of no significance under such circumstances. If the slides are scrupulously clean and the smears properly made, such cells are found only in very small numbers in normal blood. In the blood of persons who are very weary they are increased. Blood taken late in the afternoon shows a larger proportion of such cells than does morning blood, and the number in abnormal blood increases during the day and under the influence of fatigue as is the case in normal blood. Many of the functions of the white blood cells are performed through the medium of their ameboid movements. A flowing movement of protoplasm is one of the most common of vital characteristics, and by means of this property white blood cells ingest and carry fat and glycogen particles and protein molecules or radicals, thus facilitating absorption and transmission of food into the body tissues from the intestinal tract, and from one part of the body to another. By means of ameboid activity bacteria and other foreign substances are ingested, to be digested and rendered harmless. By means of the ameboid activity of blood cells, plasma cells or histiocytes, wounds are repaired, and there are other activities whose relations are not yet well understood in which phagocytosis seems to be important in physiological and pathological conditions. (Plate II) Phagocytosis and diapedesis are associated in the reactions to foreign bodies and infection. By means of diapedesis the white cells accumulate around foreign bodies and in the immediate vicinity of various abnormal tissues. The nature of the attraction exerted by irritants is not well understood. Irritation of the sensory nerve endings in the skin or mucous membranes causes considerable accumulation of white blood cells, though the affected tissues may not be reddened. The accumulation of white cells in congested areas is no doubt partly due to changes in the caliber of the blood vessels and partly to changes in the rate of blood flow, but the accumulation of white cells which occurs as a result of sensory irritation, with no recognizable vascular change, is very puzzling. Inert foreign substances inserted beneath the skin with every precaution against infection and against sensory nerve irritation of more than the faintest degree, cause their speedy congregation. Irritating substances such as croton oil or capsicum cause very rapid assembling of leucocytes in the vicinity. Injury to the cells of the body also call them together; the greater the sensory disturbance and the more complete the destruction of the tissue cells the more rapid and abundant is the gathering together of the white cells. Pathogenic bacteria, especially pyogenic bacteria associated with destruction of the tissue cells, attract them mightily. It is not to be inferred that the attraction of these substances exerts an influence over any great distance; it is enough only that the cells passing through the capillaries in the immediate vicinity of the irritant be stopped and led to pass into the tissues to secure quite rapidly a considerable crowd of white cells. Very much work needs to be done before the nature of this chemotaxis and the manner in which diapedesis occurs can be explained satisfactorily. To some extent phagocytosis is a function of all living protoplasm, since it is only by the ingestion of food materials that cells maintain life longer than for very short periods. Phagocytosis begins with the manifestations of life, in most cells, and it continues as long as cell life persists. This may be beyond the life of a multicellular body. Ameboid movements of white blood cells, for example, have been watched for five hours on the warm slide after the blood has been removed from the body. For several days after death ameboid movements of leucocytes and the waving of cilia occur in the cadaver. The term phagocytosis as employed in the study of the white cells of the body usually refers to their activities in ingesting foreign substances, and, indirectly, to such procedures for the sake of the organism as a whole in protecting the body against bacteria and other parasites, and against the effects of foreign substances or injured tissue cells within the body. Remarkable things are accomplished by means of this activity. Protection against infection is only one of the factors concerned. Malignant neoplasms often meet some such protective agencies, and large hyaline cells in many cancer cases. It is true that this activity is not sufficiently efficient to meet the situation, and that tumor growth seems to be unimpeded by the performance. It is manifestly impossible to determine whether early cancers or early metastases may be overcome by these agencies. Foreign materials of considerable size are often ingested and carried away. In one of our cases a bullet, two years within the brain, was being slowly absorbed. Minute particles of lead were found within the endothelial cells of the capillaries and the neutrophiles of the blood at a considerable distance from the bullet. In another case a small whitish mass in sputum was examined; a small bristle, probably from a toothbrush, was surrounded by phagocytes and the surface of the bristle was eroded rather deeply on all sides by these tiny scavengers. Polymorphonuclear neutrophiles resemble amebae, especially proteus, rather closely. In both cells the protoplasm is finely granular and feebly eosinophilic, and in both a very delicate intergranular hyaline protoplasm is present. The nucleus of the ameba is single and almost round while the nucleus of the leucocyte is variable in form. The nucleus of the ameba changes in form during its activity so that the resemblance is quite marked despite the more persistent nuclear polymorphism of the leucocyte. With increasing fatigue and impending death the leucocytes become vacuolated. Both amebae and leucocytes move by means of extruding masses of protoplasm called pseudopodia. In the ameba and the neutrophile, the fine hyaline protoplasm flows out first, then the granules follow, flowing into the pseudopod much as marbles might flow from one part of a loose bag into another part if the bag were pulled about over an uneven surface. In both ameba and leucocyte the nucleus remains centrally placed and always covered by a layer of protoplasm. Only under very abnormal conditions is the nucleus ever freed from its covering of protoplasm. If the temperature of the slide is raised to an abnormal degree, simulating hyperpyrexia, the protoplasm may flow away from the nucleus of the leucocyte, leaving it naked for a few seconds. Even in the presence of impending death of the cell from excessive heat, however, the protoplasm flows around the nucleus almost at once, so that the cell taken from almost or quite normal blood and subjected to excessive heat or to other very abnormal conditions on the warm stage shows almost always a rounded form in death. Naked nuclear masses sometimes are found in the blood of sick persons but it is not yet known whether these are nuclei from which the protoplasm has been carried away or has been digested, or whether they have been produced in some other manner. Upon meeting any obstacle the leucocyte ceases moving for one to several seconds. A pseudopod then is protruded laterally, the granules, the rest of the protoplasm and the nucleus flow along in the same direction and this direction is maintained until some other impediment or some force changes the direction of movement. There is no recognizable tendency for the leucocyte to turn to the left or the right. If any impediment offers a slanting surface to the advancing leucocyte the pseudopod usually is protruded along the surface of the impediment. It is possible to induce the cell to turn either to the right or to the left by obstructing its pathway by a slanting surface. No matter how oftensuch an impediment is so placed as to cause movement to the right there is no increasing tendency for a movement to occur to the right when the cell meets a surface at a right angle to its pathway; nor is it possible to cause the cell to tend to right-handed movement by repeatedly obstructing its movement. In several unicellular organisms repeated obstrauction of the movement to the right is finally followed by a marked tendency to turn to the right. No such modification of the leucocyte can be secured by conditions so far studied. The direction in which the leucocyte turns when it meets an obstruction placed directly across its path seems to depend upon the forces inherent in the cell at the instant of meeting the obstruction. If the larger moving area happens to be on the right side (the right side of the cell from the viewpoint of the observer) this mass tends to flow to the right forming a pseudopod turning to that direction. If, however, there happens to be an active mass flowing on the left side of the cell, there is a distinct tendency for the cell to turn in that direction. If a very small object, such as a grain of carmine or a bacterium, lies directly in the path of the leucocyte, the protoplasm is apt to send out two masses, usually unequal in size, and these surround and finally engulf the foreign substance. In other words, the leucocyte is positively thigmotactic. This quality is further indicated by the tendency which leucocytes have of apparently hiding beneath masses of red blood cells, on the warm stage. When the moving leucocyte encounters masses of erythrocytes it flows along the firmer surface presented by the red cells, and when the leucocyte encounters an opening between fairly firm masses of red cells and the slide or cover-glass it flows along the adjacent surfaces, thus evading further observation. Their activity is increased by increasing temperature. At a temperature of 99 degrees F. the average speed of a neutrophile is sufficient to carry it about five feet in a year. At 103 degrees F. the speed is sufficient to carry it twelve feet in a year; this speed is erratic and non-purposive, however. The rate of leucocyte motion varies in different individuals even though they are apparently in normal health. In the same individual the movements vary for different times of the day. The cells move most rapidly and begin the motions most speedily after being placed upon the warm stage in the early morning. The movements become much less active toward night and it is sometimes difficult to find any active cell in blood taken at ten or eleven oclock at night. People who are tired or who are in any way enfeebled have white blood cells which move less freely than do normal cells. These variations in the activity of the phagocytes of the blood may be one important factor in variation in immunity. Leucocytes increase in activity with increasing temperatures up to about 103 degrees F., but after that increasing temperatures decrease their activity until they die. The activity of leucocytes can be diminished or prevented by the presence of any substance not normal to the blood plasma, or by varying the concentration of the substances normal to the plasma. Increased amounts of the salts normal to the blood, or of carbon dioxide, or of urea or other non-protein nitrogenous substances diminish the activity of the leucocytes. Diluting the plasma with distilled water also diminishes or prevents leucocytic activity. The presence of oxygen is essential to normal activity. Excess of oxygen increases the activity of the white cells but diminishes their period of vitality on the warm slide. Moderate degrees of light increase their activity but direct sunlight causes speedy death, with no recognizable change in activity. Certain substances in abnormal adult human blood plasma affect the activity of the leucocytes variably. The leucocytes of an individual suffering from exophthalmic goiter, for example, show excessive activity. Certain toxic conditions are associated with abnormally increased leucocytic activity; others with diminished speed of movement. Further study is necessary before these relations can be accurately described. The ability of the neutrophiles, especially, to ingest and destroy bacteria is affected by the opsonins of the blood plasma and this ability can be studied for various basteria. The efficiency of phagocytosis for any individual at any certain time seems to depend upon many factorsthe presence of the opsonins already mentioned, the presence or the absence of fatigue toxins, of other toxic substances, of suitable nutritive materials in the blood plasma, of useful internal secretions, and probably many other factors. Immunity is, at least partly, dependent upon phagocytosis, and any factors which diminish the efficiency of phagocytosis must necessarily diminish immunity. Factors which diminish phagocytosis include almost
all kinds of toxemia and poisoning, including the presence of active drugs
and the products of abnormal metabolism. The few forms of toxemia which
cause increased leucocytic activity diminish the vitality of the leucocytes
and lead to their speedy death on the warm slide. That such poisons also
lead to speedy death within the circulatory system of the body is shown
by the presence of naked nuclear masses and of partially destroyed neutrophiles
in blood smears made for patients with such forms of toxemia.
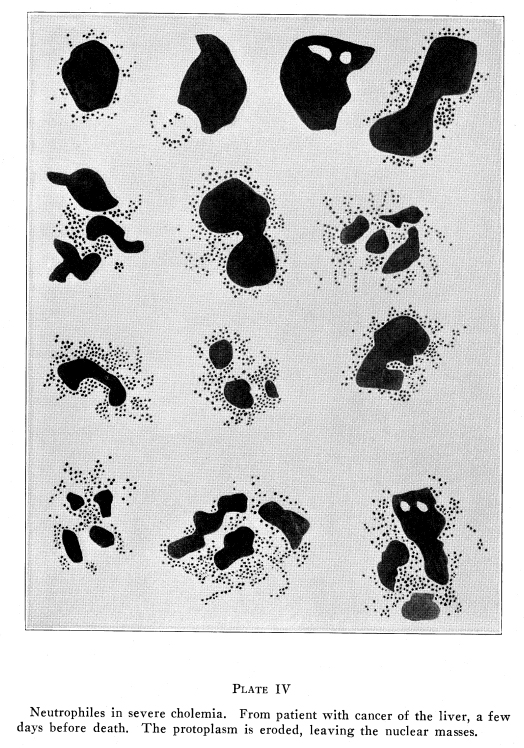
Bony lesions which interfere with the normal nutrition of the hematopoietic tissues and with those viscera which maintain a normal quality of the blood, and a normal circulation of the blood, also affect phagocytosis. Lesions of the third cervical and the second thoracic vertebrae affect the circulation through the thyroid gland and seem also to affect its nervous control, thus affecting its internal secretion. If hypothyroidism results, the white blood cells become inert but their vitality is not perceptibly affected while they are on the warm slide. If the basal metabolism is increased, the white cells show markedly increased activity and they die speedily, on the warm stage. The cells in such blood protrude two or several pseudopodia at the same time, often in different directions, and the cells behave in an erratic manner, moving different pseudopodia rapidly in different directions in turn but producing little or no efficient activity at any time. The spectacle offered by these erratic movements is very interesting. Various forms of toxemia produce similar but less marked changes in the ameboid movements of leucocytes. Fatigue of mild degree tends to increase leucocytic activity. Fatigue carried to the point of exhaustion diminishes the rate of motion of the white cells. In either case the cells die speedily on the warm slide. Lesions of the ninth and tenth thoracic vertebrae and adjacent ribs affect the circulation through the liver and permit bile pigments and sometimes bile salts to enter the circulating blood. These substances diminish the activity of the white cells and also shorten their lives on the warm slide. That such substances shorten the lives of white cells in the circulating blood also is shown by the great number of fragmented and senile cells and by the number of naked nuclear masses found in the blood in cholemia. (Plate IV) Other lesions affect ameboid movements of the white
cells chiefly by indirect means. That lesions diminish immunity in a general
way and for several types of infection has been demonstrated many times
in the laboratories of The A. T. Still Research Institute, by the speedy
death of lesioned animals whenever an accidental infection gains entrance
into the animal houses.
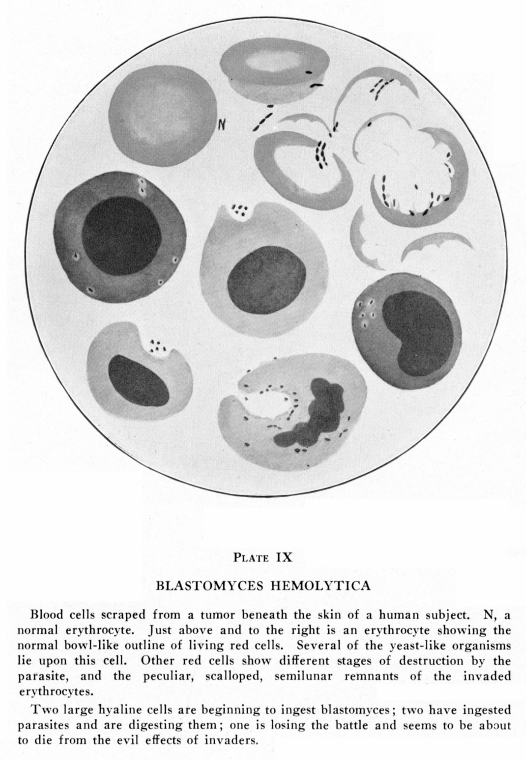
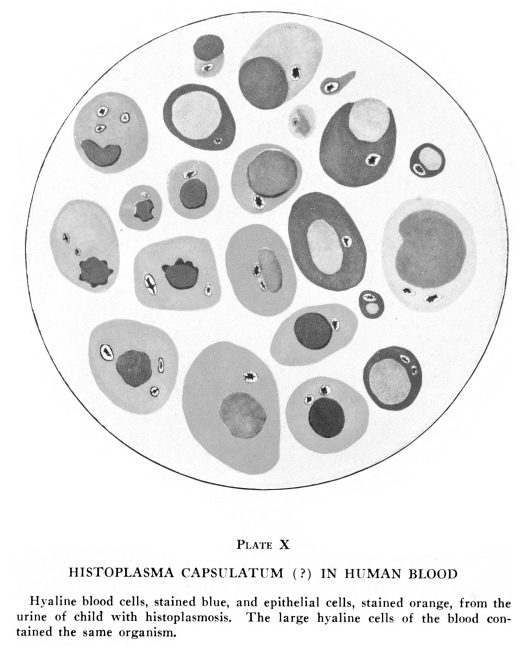
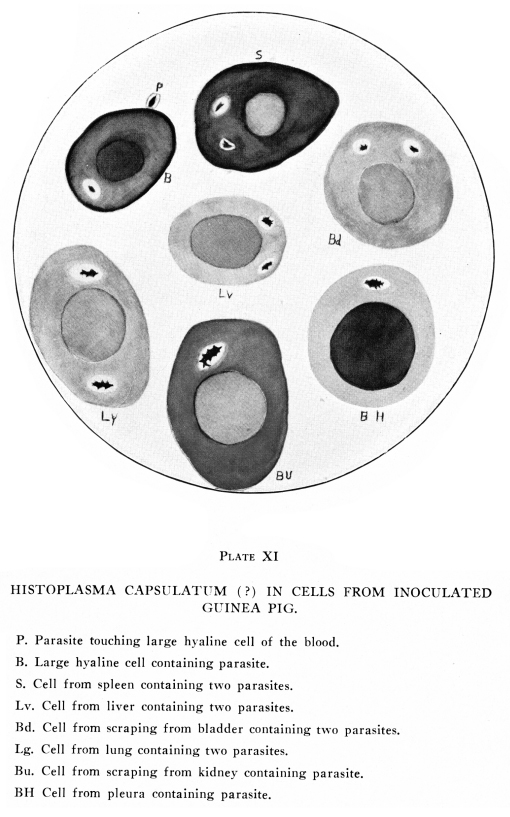
Hyaline cells are somewhat less active than neutrophiles. Their protoplasm is chiefly hyaline, though under abnormal conditions adult human blood may show granules in the protoplasm of its hyaline cells. These granules are usually of the azur type, though occasionally they may be basophilic, neutrophilic or very feebly cosinophilic, and they do not ever show any activity themselves; they act like the deutoplasm of unicellular organisms in being apparently inactive and definitely apart from the life of the cell itself. The protoplasm of the hyaline cells forms very short, blunt, heavy pseudopodia sometimes, especially if the heat of the warm slide is increased to 101 degrees F. or so. At 103 degrees F. the hyaline cells become quite active. Large hyaline cells are phagocytic for malarial plasmodia
and for certain other organisms of this general type. The histoplasma capsulata
of Darling is found almost exclusively within these cells. It is easily
recognized by its peculiar structure and by the clear space in the hyaline
protoplasm around the parasite. Large hyaline cells are phagocytic for
a few bacteria, such as the bacilli of tuberculosis and typhoid, though
they seem much less efficient as bacteriolytic agents than are the neutrophiles.
The small hyaline cells are rarely found containing either animal or bacterial
parasites. (Plates IX, X,
XI)
Eosinophiles present most interesting forms of activity. These cells have abundant large granules in their very scanty hyaline protoplasm and they are conspicuous objects on the warm slide. The granules usually obscure the thin, hyaline, intergranular substance. The granules are the active agents in their movements. The hyaline material merely follows them. The eosinophile cells alternately rest and become active and in the resting stage are round or roundish in outline. Then, for no recognizable reason, one granule rolls along the protoplasmic mass, then another and then two or three, then several, until almost the entire mass of granules is rolling along, forming pseudopodia which may become two or three times as long as the diameter of the resting cell. The nucleus is often completely left behind and it may become completely naked. But the granules do not maintain their distance for more than a few second; then one granule rolls toward the nucleus, then two or three, then several, and then the entire mass rolls back to the nucleus and surrounds it again. Then the granules usually rest for a few seconds, then the cell begins its activity again. Sometimes the granules flow more slowly and in a steadfast sort of manner; the nucleus then is carried along with the granules and the cell may thus travel over a considerable distance, though the eosinophiles are not at all likely to travel as far or as rapidly as neutrophiles do. Plate II. Eosinophiles do not seem to be phagocytic for any kind of infectious agent, nor for foreign materials left within the body. They do surround foreign materials within the body, together with the more abundant neutrophiles, and they die in great numbers around certain foreign particles, but particles of foreign matter of bacteria or other abnormal substances are not found within eosinophiles. They are probably concerned to some extent in immunity, but this function does not seem to be associated with phagocytosis. The different kinds of white cells do not react in
quite the same manner to variations in the quality of the blood plasma.
Conditions which cause increased activity of the eosinophiles may cause
diminished activity of the neutrophiles, and other conditions may cause
increased neutrophilic activity with normal or even subnormal activity
of the eosinophiles. The hyaline cells may show increased activity with
no evidence of increased activity of the granular cells. Further study
of the activities of these cells under various physiological and abnormal
conditions is necessary before these relationships can be adequately explained.
This phenomenon is visible only when the smears are correctly made so that no mechanical grouping of the cells occurs. Normally the leucocytes are not grouped in any kind of order; if two or more are close together it is accidental and their nearness due to coincidence. Under certain abnormal circumstances the blood cells are definitely grouped together, either in groups of cells classified about as shown by the differential count, or as groups of cells of a single type. This grouping is often quite intimate, so much so that the cells may seem on the point of conjugating or of separating after cell division. More commonly the cells merely lie close together in the smear or on the warm slide. It may be noticed while watching the movements of the cells on the warm stage that there seems to be an attraction of one cell to another cell and that these tend to approach one another. Usually this appearance of mutual attraction disappears before the cells come in contact; occasionally they become closely approximated and exert more than the original attraction for other leucocytes which are in the immediate locality. This attraction is not universal, for often one cell will fail to attract a certain cell but will definitely attract a third or fourth cell. Two cells of the same class may be attracted or two cells of different classes. The eosinophile and the endothelial cell seem to exert little attraction for other cells and are not often attracted by them. Eosinophiles are often grouped together and endothelial cells may be arranged in definite masses. Neutrophiles are most commonly found in groups, though this may be partly on account of their relative numbers. Lymphocytes are concerned in grouping, but only with neutrophiles and within their own class. In the stained smears more definite information is
secured because the smears are more even than is the case with warm slide
preparations. Here the cells may be arranged in quite large groups either
of the same or of different classes. The cells are usually not very closely
approximated but they lie in definite groups.
The cause of this grouping is not known. It is not due to any particular stickiness of the cell protoplasm because the cells do not merely adhere, they are definitely attracted and move toward one another on the warm slide. They are rarely actually in contact, which also precludes the idea that increased stickiness of the protoplasm is a factor in causing the condition. Cells which are gregarious seem to be less active in phagocytosis than normal cells. Bacteria, foreign bodies and pigment granules are less commonly found within them than within cells of the same types but not showing this peculiar phenomenon of gregariousness. Gregariousness adds gloom to the prognosis in any condition with which it is associated. In pneumonia the appearance of definite gregariousness indicates that the heart is becoming affected. In any acute infection, the sudden appearance of gregariousness suggests cardiac inefficiency. In cardiac diseases some degree of gregariousness is always present, and a sudden increase in the grouping of the cells indicates impending failure. Gregriousness of mild degree may be present in mild circulatory disturbances, such as might be caused from cardiac neuroses or from local vasomotor disturbances. Bony lesions cause local circulatory disturbances in certain viscera, and some mild gregariousness due to such lesions is often found in blood which shows no evidence of organic disease The cells return to their normal relations within ten days or two weeks after the correction of the lesions. The location of the area of inefficient circulation may sometimes be suggested by factors associated with the gregariousness. For example, if gregariousness of mild degree is present in the blood of a patient with no definite symptoms of organic disease and without any definite increase in the red or white cell count, or any considerable variation from the normal differential counting, serious organic disease is not indicated, but some area of disturbed circulation is very strongly suspected. If in such a case there should be a trace of bile pigments in the plasma, beyond the very faint trace which is probably normal, then some circulatory disturbance of the liver is suspected. If the blood in such a case contained a slight excess of eosinophiles, and if these were definitely myelocytoid, with rather marked intergranular, basophilic, hyaline protoplasm, then it is suspected that the pelvic tissues (ovaries, testes, prostate) suffer from disturbed circulation. If the blood in such a case shows no evidence of anemia, and still contains occasional normoblasts or reticulated erythrocytes, or if there are many immature or myelocytoid granular cells, then it may be concluded that there is some considerable area of red bone marrow concerned in the circulatory inefficiency. If gregariousness occurs in blood which shows also a rather high red and white cell count, then cardiac weakness is strongly suspected. The heart may not be organically diseased, but there is certainly some abnormal condition affecting the cardiac function in such a case. Lesions of the third or fourth thoracic vertebrae cause cardiac weakness in laboratory animals, and the blood of these animals shows gregariousness which is chiefly marked in the hyaline cells. When marked gregariousness occurs in the blood in
any of the chronic diseases, or when there is a sudden appearance of gregariousness
in blood which previously has not shown this characteristic, then an exacerbation
of the disease or impending cardiac failure is to be expected. Sudden appearance
of marked gregariousness in the blood of any person indicates the onset
of some serious state, and if that person is already ill it often indicates
impending death. This is especially noticeable in cases of leukemia, pernicious
anemia, heart disease and pneumonia.
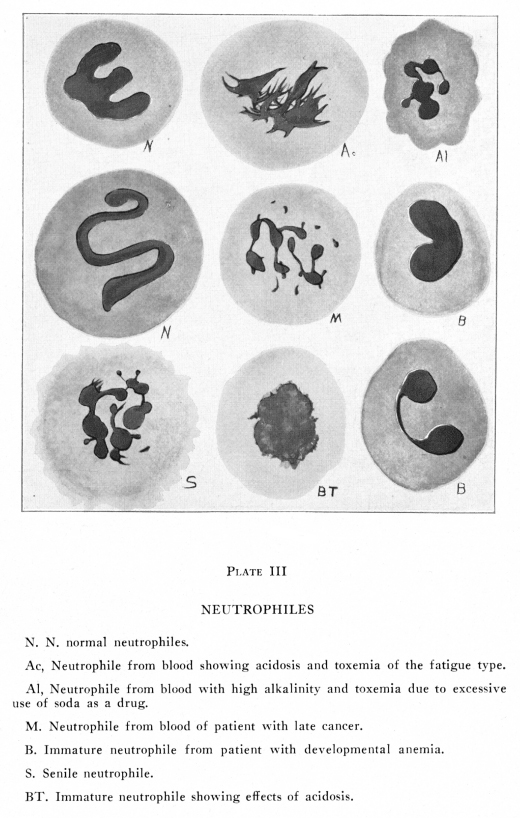
The leucocytes are variously affected by toxemias. Typical changes occur in acidosis, alkalosis, fatigue, cholemia, senility and disturbances in protein katabolism. In acidosis associated with excess of carbon dioxide in the blood stream there is a slight but definite swelling of all the blood cells. The erythrocytes are larger than normal by about one-half micron in diameter. The leucocytes are enlarged by one to four microns in diameter as they appear on the warm slide. All the blood cells lie flatter on the slide, and they seem flabbier than normal. The nuclei take stains with less avidity and they show a grayish tint instead of the normal bright blue in eosin-methylene blue stains. The nuclei are somewhat larger than normal and they are occasionally vacuolated. The chromatin masses are less distinct and are somewhat smaller than normal. These findings apply to all the nuclei of the white cells in the blood of a patient with acidosis. The neutrophile protoplasm stains less vividly than normal, and the granules show greater variation in size than in normal blood. The edges of the neutrophiles are often ragged and frayed in appearance. The limiting layer of the cell seems to be in solution so that the protoplacsm merges into the plasma without definition. The eosinophiles stain with less than normal avidity, and the eosinophile granules seem less definitely spherical than normal. The hyaline cells stain less vividly than normal and their edges also are indistinct, though the fraying is less marked than in neutrophiles. The leucocytes move sluggishly on the warm slide
and they die within half an hour at most.
In alkalosis the nuclei stain with unusual brilliance. In Giemsa staining the nuclei show a more distinct purplish tone than is the case with normal blood. The nuclei are slightly shrunken and they seem to have a thickened nuclear membrane. The chromatin masses are large, distinct, and deeply stained. All the cells are diminished in diameter and all
seem to be more definitely spherical than normal. The cell outlines are
distinct and very often there is a peripheral condensation of protoplasm
suggesting a definite cell wall. The granules of the neutrophiles are brilliantly
stained in eosin-methylene blue preparations and they take eosin more avidly
than do normal neutrophiles. The eosinophile granules stain vividly and
they seem to have a higher refrangibility than in normal blood.
In severe acute fatigue the changes are less marked than in chronic fatigue. Fatigue is usually associated with some degree of acidosis and the changes already described for acidosis are present in fatigue. To these are added other changes. The granules of the neutrophiles are smaller than normal and may be fine and dust-like. Their outlines are very indistinct. The nuclei are more swollen in severe fatigue than in acidosis and the nuclear outlines are more irregular. Very often considerable areas of the nuclear periphery are frayed out into a fringe-like margin. The outlines of the hyaline cells are more ragged than is the case in acidosis and they show considerable variations in staining reactions. Monocytes are usually increased in fatigue. After very severe acute fatigue there may be considerable numbers of endothelial cells present. In severe chronic fatigue there may be many naked nuclear masses present in the blood smears, and these may occasionally retain a few very small masses of protoplasm which identifies the nature of the original cells. Such nuclear masses seem to be derived from all the leucocyte groups as a result of the disintegration of their protoplasm. The cells show little movement on the warm slide, in severe or chronic fatigue, and they often begin to die almost at once. In mild acute fatigue the cells begin to move at once and show remarkably increased activity. Their pseudopodia are long and sprawling and are protruded and retracted in different directions, in a peculiarly purposeless manner. They begin to due within ten to thirty minutes. With rest the cells regain normal activity. It is
impossible to determine whether cells once seriously affected regain normal
functions or not. Since the lifetime of the leucocytes is certainly very
short it may be that the leucocytes once affected by the toxins present
in acute fatigue perish and are replaced by others which develop in the
rested body and are, therefore, unaffected. In chronic fatigue the newly
developed cells are also affected by the toxins constantly present in the
blood plasma.
The presence of bile salts or acids in the blood stream exerts a destructive effect upon all blood cells. The red blood cells show speedy laking on the warm slide, and the stained smears show many fragmented erythrocytes. The red cells are fragile and inelastic. Blood shadows (red blood cell stromata from which the hemoglobin has been dissolved) are present, sometimes in considerable numbers. The protoplasm is often disintegrated to such an extent that it may be impossible to make a satisfactory differential count in severe cases of cholemia. Vacuoles are often found in the protoplasm and in the nuclei of the neutrophiles, and in the nuclei of the eosinophiles. The eosinophile granules are not affected. The staining reactions of the nuclei are not affected. The hyaline cells are affected less seriously than the neutrophiles, but their protoplasm is often ragged around the edges if the cholemia has been present for some weeks. (Plates III, IV, XIII) Plate II
The toxic products of abnormal degeneration of protein substances may be absorbed into the blood and may affect the blood cells quite seriously. The red cells show little or no ill effects of this form of toxemia unless anemia supervenes. The neutrophiles show the most marked effects. Their nuclei present extremes of polymorphism and small aberrant masses of nuclear substance may occasionally be found in the protoplasm near the periphery of the cell. The nuclei themselves remain near the central area of the cell. The edges of the nuclei are definite and distinct, as in alkalosis. From this edge there are peculiar prolongations somewhat resembling pseudopodia except that the ends are often broadened out into knob-like structures. These nuclear pseudopodia have distinct outlines and do not in the least resemble the fringelike frayed edges of the nuclei found in fatigue or acidosis. Vacuoles are not found in the nuclei in typical cases. The nuclei of the eosinophiles and of the hyaline cells rarely show the nuclear pseudopodia which are so conspicuous in the neutrophiles, but they often are divided into two or more definite masses. The lymphocytes often contain two nuclei but it is extremely rare that evidences of cell division are found in these cells. The monocytes are increased in number and they often contain granules which seem to be deutoplasmic and are probably formed from ingested protein materials derived from the degenerating tissues or fluids. The fibrin threads appear upon the warm slide more abundantly and more speedily than they do in normal blood. The threads are irregular in outline, are often beaded and they may form peculiar, radiating, net-like or felt-like structures. In the absorption of pneumonia exudates and during the very early stages of pneumonia the threads are very long, very abundant, very quickly formed, regular in contour and they form heavy, felt-like masses. In carcinoma they are more often radiating and the threads are much more irregular in contour. Small, highly refractile granules are usually abundant on the warm slide and they stain in different ways according to their chemical nature. Some of these are lipoid or fatty, and they stain with Sudan III or osmic acid; these granules are present only when there is some degeneration of protein substances. Others give a brownish, reddish or bluish color with iodine; these also are present when protein substances are being broken down into glycogen or some related substance. Other granules do not stain by ordinary methods; they include several different compounds such as granules from disintegrated leucocytes, tissues, fluids and other protein substances. The sudanophilic and iodophilic granules are recognizable within the hyaline cells and the neutrophiles. Toxemia of this type is always associated with some
absorption of abnormal protein katabolites. Individuals with any kind of
intestinal putrefaction and who eat excessively of high-purin foods often
absorb toxic substances which produce this blood picture. The stage of
resolution and absorption after pneumonia may be characterized by the same
findings. A degenerating benign neoplasm may also cause sufficient toxemia
to bring about these same changes. The most marked form of this type of
toxemia occurs during the rapid growth of a malignant neoplasm or the absorption
of fluids from a cyst or from peritoneal or pleural exudates. Carcinoma
produces more definite findings than any other neoplasm.
In old age or in premature senility the neutrophiles show characteristic changes. The granules are fine, often dust-like, and they stain feebly. The nuclei of all leucocytes stain feebly. Vacuolated swollen nuclei and nuclei with frayed outlines are abundant. Polymorphism of the nuclei of neutrophiles, eosinophiles and large hyaline cells is pronounced. The lymphocytes often contain two nuclei. A peculiarity of the nuclei of the leucocytes of
senility is the presence of shrunken nuclei in which the chromatin forms
large masses which stain with unusual avidity.
|
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}