General.
A systematic treatment of radiation physics would
be beyond the scope of this book. It is assumed that the reader has
a general understanding of such matters as the theory of electro-magnetic
vibrations, the transformation of these vibrations into other forms of
energy when they are absorbed, and the common units of measurements used
in electrical work. A short list of recent books and papers is given
which will assist further reading in these subjects in connection with
light therapy.
Units and Constants.
The following data are stated for reference:
Spectrum wave-lengths:
| 1 A. U. (Angstrom Unit) | =1 mm./10,000,000 | (10-7 millimetre). |
| 1 uu (millimicron) | = 1 u/1,000 | (10-6 millimetre). |
| 1 u (micron) | = 1 mm./1,000 | (10-3 millimetre). |
Speed of Transmission: (Velocity of light, uniform for all electro-magnetic vibraitons) = 300,000 kilometres per second.
Electrical units:
Volt = Unit of electro-motive force (i.e., that pressure
which will cause a current of 1 ampere to flow against a resistance of
1 ohm.
Ampere = Unit of rate of transfer of electricity.
Watt = Unit of quantity of electricity transferred,
i.e., the amount of current consumed when a current of 1 ampere flows at
a pressure of 1 volt.
Ohm = Unit of resistance to electric flow, i.e.,
the resistance of a column of mercury 106.245 cm. long X 1 mm. diameter
at 0 degrees C.
Radiations used in Actinotherapy.
The groups of electro-magnetic vibrations used in
actinotherapy are:
|
|
|
|
| Ultra-violet rays | ||
| 1850 16 X 10/14/sec. | Limit of transmission for quartz. | |
| Short region | ||
| 2200 13.5 X 10/14/sec. | ||
| Middle region | The erythema producing rays. | |
| 3130 9.5 X 10/14/sec. | ||
| Near region | Pigmenting rays. | |
| 3900 7.5 X 10/14/sec. | ||
| Visible rays | ||
| 7600 4 X 10/14/sec. | ||
| Infra-red | ||
| (near region) | Rays of deep penetration. | |
| 15000 2 X 10/14/sec. | ||
| (long rays) | Little penetrating effect. | |
| 40000 7.5 X 10/13/sec. |
A certain aspect of radiation physics which has special
significance for the practitioner of actinotherapy is considered in outline
here, i.e., the output of different sources in the various spectrum regions.
The spectrum photograph of any source gives merely a qualitative indication
of its emitted energy. It is necessary to know also how the total
energy radiated is divided between the different parts of the spectrum.
To determine this accurately requires the resources of a specially equipped
physical laboratory. For practical use in actinotherapy the problem
narrows down to estimating dosage in terms of biological reactions to certain
short wave-lengths. This makes it practicable to estimate the output
of a source either by physical methods (spectroscopy, photolytic measurement)
or by biological estimation (erythema reaction, bactericidal effects, etc.).
A classified list of recent publications on the subject will be found on
page 15 (8-33).
The energy distribution of the quartz mercury arc
and other standard sources used in therapy are well established, and the
user can rely on approximately constant energy distribution, provided that
lamps are operated to instructions. Most users find it sufficient
to standardize their lamps by occasional erythema lists on a standard subject,
or by a simple gauge such as the actinometers specifically designed for
use with quartz lamps.
Output Characteristics of Standard Lamps.
For effective use in actinotherapy, a source must
generate adequate total radiation. Further, a sufficient proportion
of this total must be generated in the required section of the spectrum.
For the standard sources discussed in this book, the output characteristics
are:
|
|
|
|
|
| Sollux Lamp (9) |
|
|
|
| Quartz Mercury Arc
air-cooled (41 43a). |
|
|
|
(See output diagram, page 18.)
The distribution characteristics of a quartz burner
are practically constant throughout its operating life. An aged burner
shows decrease in total output, which affects both the short and long ultra-violet
and the visible spectrum in a nearly equal measure (Anderson). A
list of recent technical papers on the mercury vapour arc will be found
on page 16 (34-43a).
Filters and Screens.
The human eye is very sensitive to the short ultra-violet rays below 3150 A.U. It is essential to use goggles which completely protect the eyeball, or efficient screens, when using ultra-violet sources. Most commercial glasses, in adequate thickness, are opaque to the irritant rays, and therefore safe as screens.
Filters.
In certain therapeutic and other applications, the
need arises for filters which will transmit certain portions of the spectrum.
Following are transmission data for the filters mentioned in this book:--
| Filter. | Uses. | Spectrum Limits (A.U.) | |
| Short. | Long. | ||
| "Diagnosis" | Fluorescence (excluding visible light). | 3000 -- | 4000 |
| maximum at 3660 | |||
| "Uviol White"
(2 mm.) |
Exclusion of shortest ultra-violet rays. | 2600 -- | |
| "Uviol Blue"
(2 mm.) |
Exclusion of shortest ultra-violet rays. | 2750 -- | 5000 |
| (6550 -- 30,000) | |||
| Sollux Red
(2mm.) |
Red and infra-red radiation. | 6000 -- | |
| Sollux Blue
(2mm.) |
Blue and infra-red radiation. | 3010 -- | 4550 |
Physics in General.
1. Harris, D.T. -- Technique of Ultra-violet Radiology
(19332 6/-).
2. Luckeish, M. -- Ultra-violet radiation, its properties,
production, measurement and applications (1923, 21/-).
3. Anderson, W.T. -- Quartz Lamp, August,
1923 -- March 1924.
4. Goodman, H. -- Trans. Illum. Eng. Soc. (N.Y.),
April, 1927.
5. Hauer, F. -- Die kunstlichen Lichtquellen (in
Handbuch der Lichttherpie, ed. Hausmann & Volk), 1927.
6. Hopwood, F.L -- Nature, April 21st, 1928.
7. Hibben, J.H. -- Med. Jnl. and Record,
April 1st, 1931.
Also Nos. 785
787 790 792
Determination of Actinic Output.
General.
8. Baly, E. C. C. -- Spectroscopy, Vols. 1-2 (1924-1927.).
9. Ryde, J. E. -- Elec. Rev., June 5th, 1925.
9a Nogier, T. -- Phys. Therapeutics, October,
1926.
10. Finkenrath, K. -- Zentrablatt F. Haut-Krankheiten,
1927, 15, No. 7. (Contain a summary of papers prior to 1924.)
11. Halban, H. & Eisenbrand, J. -- Proc.
Royal Society, A., 116, 1927, 153-160.
12. Estey, R. S. -- Med. Jnl. and Record,
December 17th, 1930. (See also list of works under Dosage, Nos. 141 to
152.)
Photometric Measurement.
13. Anderson, W. T. & Gordon, E. -- Jnl. Optical Soc. America, March 1928.
Photo-Chemical Measurement.
14. Bering, F. & Meyer, H. -- Strahlentherapie,
1912, No. 1-2.
15. Keller, P. -- Klin. Ws., 1924, No. 37.
16. Webster, A., Hill, L. & Eidinow, A. -- Lancet,
1924, l, 745.
17. Anderson, W. T. & Robinson, F. W. -- Jnl.
Amer. Chem. Soc., March, 1925.
18. Pohle, E. A. -- Jnl. A.M.A., March 20th,
1926.
19. Moss, J. E. & Knapp, A. W. -- Brit. Jnl.
Actinotherapy, January 1927.
20. Gillam, A. E. & Morton, R. A. -- Jnl.
Soc. Chem. Industry, 46, 1927, No. 44.
21. Hauer, F. -- Methoden der Lichtmessung im Ultraviolett
(in Handbuch der Lichttherapie, ed. Hausmann & Volk, 1927).
22. Morton, R. A. -- Radiation in Chemistry (12928,
12/6), Chapters 3, 6.
Photo-Electric Measurement.
23. Dorno, C. -- Strahlentherapie, 14, 1922,
No. 1.
24. Peemoller, F. & Dannmeyer, F. -- Med.
Klinik, 1923, No. 29.
25. Griffith, H. D. & Taylor, J. S. -- Lancet,
December 5th, 1925.
26. Dannmeyer, F. -- Strahlentherapie, 22,
1926, 738-750.
27. Ruttenauer, A. -- Strahlentherapie, 27,
1928, 794-799.
28. Harris, D. T. -- Jnl, Sci. Instruments,
January, 1929.
29. Goodman, H. -- Phys. Therapeutics, February
1929.
Biological Estimation.
30. Coblentz, W. W. -- Amer. Jnl. Electrotherapeutics,
July, 1925.
31. Peacock, P. R. -- Lancet, August 22nd,
1925.
32. Bridge, E. -- Med. Jnl. and Record, December
4th, 1929.
33. Waller, M.D. -- Proc. Royal Society,
B., 108, 1931, 264-270 (Quartz Lamp, S., October, 1931).
The Mercury Vapour Arc.
34. Johannsen -- Strahlentherapie, 1915, 45.
34a. Coblentz, W. W. -- Amer. Jnl. Electrotherapeutics,
October, 1921.
35. Watters, B. D. H. -- Phil. Mag., September,
1924.
36. Coblentz, W. W. -- Amer. Jnl. Electrotherapeutics,
December, 1925.
37. Reeve, L. -- Jnl. Phys. Chemistry, January,
1925.
38. Drane, H. D. H. -- Brit. Jnl. Actinotherapy,
June, 1926.
39. Gillam, A. E. & Morton, R. A. -- Phil.
Mag., December, 1928.
40. Coblentz, W. W. -- Jnl. Amer. Med. Ass.,
June 1st, 1929.
41. Anderson, W. T. -- Radiology, July, 1930
(Quartz Lamp, S., October, 1931).
42. Anderson, W. T. -- Med. Jnl. and Record,
December 17th, 1930 (Quartz Lamp, January 1931).
43. Dingee, A. L. M. -- Phys. Therapeutics,
May, 1930.
44. McAlister, E. D. -- Absolute intensities in
the visible and ultra-violet spectrum of a quartz mercury are (Smithsonian
Institution, 1933).
Filters and Screens.
44. Watters, F. D. H. -- Lancet, September
5th, 1925.
45. Goodman, H. & Anderson, W. T. -- Boston
Med. and Surg. Jnl., January 12th, 1928 (Quartz Lamp, February, 1928).
46. Watters, B. D. H. -- Brit. Jnl. Actinotherapy,
August, 1929.
47. Coblentz, W. W. -- Journ. A.M.A., Sept.
20th, 1930 (Quartz Lamp, December, 1930).
48. Ross-Mansell, J. -- Optician, May 8th,
1931.
49. Grant, J. -- Glass, September, 1932.
Also Nos. 2 783
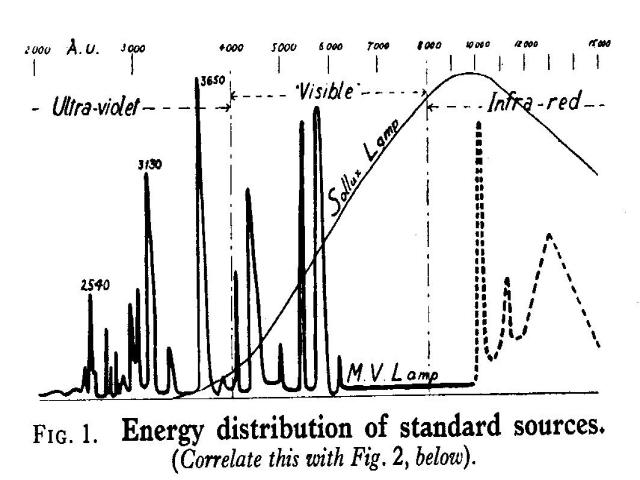
| FIG. 1. Energy distribution of standard sources.
(Correlate this with Fig. 2, below) Heavy line: The mercury vapour are in quartz. (The Alpine Sun Lamp radiation extends into the infra-red region up to 15,000 A.U. and beyond). The Kromayer Lamp radiation is weakened from 8,000 A.U. upwards through absorption by water, and ends about 14,000 A.U.; shown dotted above. Light line: The Sollux Lamp. (Data supplied by Dr. W. T. Anderson). |
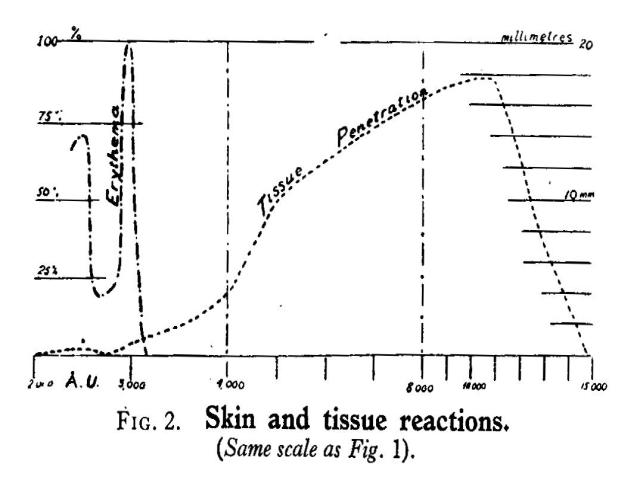
| FIG. 2 Skin and tissue reactions.
(Same scale as Fig. 1). (a) Skin erythema reaction, expressed in arbitrary units (Hausser & Vahle). (b) Tissue penetration of different wave lengths expressed in mm. (Anderson). |
Penetration of the Skin.
Penetration is an important factor. When the skin is dehaematized by compression, penetration may be increased; otherwise, all rays shorter than 3000 A.U. are absorbed by 1 mm. thickness of skin. The longer ultra-violet rays (over 3000 A.U.) have somewhat greater penetration, but are all absorbed between the stratum corneum and the dermis.
Rost (132) states the absorption of ultra-violet rays in the various
skin strata:
| S. corneum | --- | some fluorescence. |
| S. lucidum | --- | little action observed. |
| S. granulosum | --- | little action observed. |
| S. germinativum | --- | absorption: reaction (pigment formation). |
| Papillae | --- | endothelial absorption: vascular enlargement: erythema. |
| Corium | --- | direct absorption by capillaries (assumed but not demonstrated). |
Effects on the Skin.
The local reaction of the skin to actinic rays is
the latent erythema which develops after a few hours. The latent period
varies inversely with the exposure (63 81) and may range from 1 to 8 hours.
The erythema is not a primary but a secondary reaction, associated with
increase of temperature and emission of heat by the skin.
The wave-lengths most active in producing erythema
are those below 3200, with maxima about 2970 and 2500 A.U. (see the diagram
on page 18).
The erythema reaches its maximum 8 to 24 hours after
exposure, and then subsides. A mild erythema (first degree) may practically
disappear within 24 hours. There are great individual variations in the
onset, peak, and total duration of erythema reactions; Schall and Alius
have studied these in detail (68 69 76).
Histologically, the erythema is associated with
enlargement of the capillary vessels, which are filled with erythrocytes,
and with leucocytosis in the irradiated area. The inflammatory reaction
is not confined to the irradiated surface, but extends deeply into the
tissues.
In relatively few conditions (ulcers, wounds, dermatomycoses)
is the direct bactericidal action of light exercised on the human body.
Actinic irradiation takes effect primarily on the skin functions, which
in time set up secondary reactions in the organism as a whole.
Memmesheimer (77) explains the process as follows:
-- The skin is conceived as a gland with internal secretions, which are
of importance in the defensive mechanism of the body ("esophylaxis"). Under
the stimulus of actinic rays the walls of the skin-cells in the absorbed
layers become permeable, and substances pass from the activated cells outward
into the blood. These substances (the so-called "detoxin") consist of tyrosin
and other amino-acids. They promote increase of antibodies in the blood.
Other substances transmitted from the irradiated
skin-cells into the blood resemble histamine in their action.
Very powerful local erythema (dermatitis bullosa)
releases products of inflammation from the cells which have the same effect
as parenteral proteins (831).
Pronounced erythema is followed by desquamation.
A severe (fourth degree) erythema will produce blisters, due to exudation
of leucocytes between the horny and granular layers of the epidermis; these
heal without scars.
Pigmentation is due to the production of oxydase
ferment ("dopa") by the skin cells during the regenerative phase which
succeeds their first response to light stimulus. This ferment leads to
the formation of melanin caps on the epithelial and basal cells of the
epidermis. Pigmentation and erythema, although often associated, are not
inter-dependent; pigmentation is produced by longer-waved radiations than
the erythema-causing band. The function of pigment is disputed; Rost (132)
and other authorities assert that repetition of the erythema reaction,
avoiding pigmentation, produces best results. References 65 77 (page 28)
show the most important recent publications on this aspect.
Fluorescence.
For a detailed summary of the use of fluorescent
rays in the examination of blood, urine, bile, and of internal organs,
the work of Radley & Grant (88) should be consulted.
In medicine, the chief application of fluorescence
has been in the field of dermatological diagnosis. The detection of ringworm
by its vivid green fluorescence is now routine procedure (see references
under Tinea, Nos. 641 to 650). Many other skin diseases also show characteristic
fluorescences which are valuable aids in diagnosis.
Goodman (85) gives a useful list of characteristic
fluorescences from which the following are extracted:--
Keratosis -- white underlying fluorescence.
Leucoderma -- white in vivid contrast to surrounding
skin.
Pityriasis versicolor (microsporon furfur) -- dull
golden yellow glow.
X-ray dermatitis -- marked fluorescence in patches,
dark elsewhere.
Other authorities mention favus, impetigo, psoriasis
(which gives a silvery appearance), as readily diagnosed by their fluorescence.
Anomalies such as eczematous changes and incipient
X-ray dermatitis can be detected by fluorescence at a stage when they are
invisible by ordinary illumination. Changes in teeth, hair, and other structures
are more visible under the invisible rays than in daylight.
Effects on the Blood.
Experiments and clinical findings indicate that actinic
radiation produces considerable changes, most probably indirect, on the
blood and haemotaopoietic organs. Although there is some discordance in
the recorded results, probably due to the different light sources utilized
and to variations in the subjects, it is clearly established that blood-regeneration
in anaemic conditions takes place more rapidly under irradiation than in
its absence. The characteristic changes in the blood picture are probably
developed by way of the sympathetic nervous system (595).
There is marked action on the white blood cells.
The erythema-producing rays produce leucocytosis and lymphocytosis, with
a shift in the differential leucocyte court (increase in polymorph cells).
The maximum change occurs about 4-5 hours after irradiation; there is usually
a return to normal within 4-5 days. The red cell count and haemoglobin
content show increase after irradiation, particularly when sub-normal at
the outset.
The erythema-producing rays, in normal dosage, evoke
a rise in the bactericidal power of the blood. (It is stated that over-dosage
may reverse this effect) (92). Probably associated with this factor is
the increased resistance to infection of various kinds, e.g., staphylococcus
(106), colds (273), diphtheria (91), which follows actinic irradiation.
Huntermuller (109) has measured a three-fold increase in the alexines after
light baths.
Other recorded changes in the blood picture after
irradiation include: -- Reduction in alkalinity (96); shortening of bleeding
time (102); increase in serum mineral content (calcium, phosphorus, iron,
iodine); decrease in blood sugar.
Associated with the vascular dilation is a reduction
of high blood pressure, often considerable in extent (796).
It cannot be said that the important subject of
blood reactions is yet satisfactorily understood. References 89-112 (page
29) will assist further reading.
Effects on Metabolism.
Actinic irradiation with the short ultra-violet rays
(below 3020 A.U.) creates Vitamin D in the human body, raises the serum
content of calcium and phosphorus, and promotes the fixation of these minerals
in the body. It is thus of special value in conditions of calcium deficiency
(rickets, tetany, osteomalacia) and during times of abnormal calcium demand
(e.g. pregnancy).
Irradiation produces other changes in metabolism,
likewise important in their results but less well explained. Some are probably
indirect effects of exposure to light, conditioned through the sympathetic
nervous system. There is considerable discordance between different observers'
reports, due probably to inevitable differences in subjects, sources, intensity
of exposures, and other variables.
Respiration is decreased in frequency and increased
in depth, with a net rise in minute-volume. Intake of oxygen and output
of CO2 show increase.
Both anabolism and catabolism appear to undergo
stimulation through light. This leads in practice to the paradox that irradiation
will both reduce obese and develop thin subjects.
Irradiation has also considerable effects on the
carbohydrate metabolism. There is increase both in mobilisation and combustion
of blood sugar, and parallel to this proceeds a reduction both of glycosuria
and of acetone body excretion in diabetic subjects.
For some days following a general light bath, there
is considerable increase in excretion of nitrogen, phosphorus, sulphur
and salt, indicating enhanced activity in albumen metabolism. Many reports
indicate increased fixation of iron after irradiation, and the iodine content
of the thyroid also shows some rise.
Ultra-violet radiation has a stimulating and regulating
effect on the endocrine glands, and assists the production of hormones.
Thus, the effects of endocrine therapy are increased by concurrent irradiation.
General.
Among the physiological effects of irradiation should
also be mentioned its effects on the nervous system. It acts on the sympathetic
system, and so affects the respiration and the endocrine glands. Again,
it has marked analgesic effects, probably due to action of the rays on
the peripheral nerve terminals.
The following summary of physiological reactions
is given for reference:--
(a) Direct Effects.
Direct bactericidal action on surface infections.
Stimulus of skin cells and increase in their oxygen-metabolism.
Release of endogenous proteins and other substances
into circulation (after severe dose).
Formation of vitamins or pro-vitamins.
Erythema, some hours after irradiation, with dilation
of the superficial blood vessels, increase in skin temperature and vasomotor
activity. Erythema is not usually observed in infants.
Improvement of skin tone, and increased firmness
and development of the underlying musculature. Increased "esophylaxis"
(anti-body forming function of the skin).
Stimulation of the skin functions (transpiration,
heat regulation, resistance to infection).
Pigmentation (after a series of increasing exposures).
(b) Effects on the Blood through the Skin.
Increased content of calcium, phosphorus, iron and
iodine.
Increase in the bactericidal power (originating
locally in irradiated area).
Increase in haemoglobin and red corpuscles.
Lymphocytosis and leucocytosis.
Normalization of blood pressure.
(c) General Effects on the Body.
Increased metabolism, shown in improved appetite
and sleep, increased assimilaton and diuresis.
Marked mental stimulation, through action on the
central nervous system.
Reduction of pain through analgesic effect on the
peripheral nervous system.
Deepening and slowing of respiration, with increased
expiration of carbon dioxide.
REFERENCES TO LITERATURE.
Penetration.
50. Macht, D. I., et al. -- Proc. Soc. Exper.
Biology, 1925, 23, No. 5 (Quartz Lamp, February, 1926).
51. Schultze, W. & Rothmann, S. -- Strahlentherapie,
1926, 22, p. 736.
52. Stenstrom, W. & Reinhard, M. -- Acta
Radiologica, 1926, 5, p. 552 (Brit. Jnl. Actinotherapy,
April 1927).
53. Reis, J. v. -- Schweiz. Med. Ws., March
12th, 1927, p 248.
54. Anderson, W. T. & Macht, D. I. -- Amer.
Jnl. Physiology, September, 1928, and Brit. Jnl. Actinotherapy,
October, 1928.
55. Macht, D. I., Anderson, W. T. & Bell, F.
K. -- Jnl. A.M.A., January 21st, 1928.
56. Bachem, A. & Kunz, J. -- Archives Phys.
Therapy, February, 1929.
57. Bachem, A. & Reed, C. I. -- Amer. Jnl.
Physiology, November, 1929 (Quartz Lamp, N., July, 1931).
58. Bachem, A. -- Amer. Jnl. Physiology,
December, 1929 (Quartz Lamp, N., September, 1931).
59. Hill, L. -- Med. Press, June 11th, 18,
1930 (Quartz Lamp, S., October, 1931).
60. Takahashi, T. -- Brit. Jnl. Phys. Med.,
July and August, 1930.
61. Anderson, W. T. & Fraser, H. D. -- Brit.
Jnl. Phys. Med., November 1931.
62. Bachem, A. & Reed, C. I. -- Amer. Jnl.
Physiology, April, 1931 (Quartz Lamp, N., June 1931).
63. Lucas, N.S. -- Biochem. Jnl., 25, 1931,
No. 1.
64. Pearson, A. R. & Gair, C. J. D. -- Brit.
Jnl. Phys. Med., May 1931.
Also Nos. 132 177
Skin Effects.
65. Hausser, K. W. & Vahle, W. -- Strahlentherapie,
1922, 13, 41-71.
66. Hausmann, W. -- Strahlentherapie, 1923,
Suppl. 8, p. 126 (Quartz Lamp, February, 1924).
67. Moncorps, C. -- Munch. Med. Ws.,
1924, No. 30.
68. Schall, L. & Alius, H.J. -- Strahlentherapie,
19, 1925.
69. Schall, L. & Alius, H. J. -- Strahlentherapie,
23, 1926, p. 161-180.
70. Schultze, W. & Rothmann, S. -- Strahlentherapie,
22, 1926, 736-737.
71. Hausser, K. W. & Vable, W. -- Siemens
Wiss, Veroffentl., 6, 1927.
72. Politzer, G. -- Die morphologischen lichtbewerkten
Veranderungen normaler und errankter Gewebe (in Handbuch der Lichttherapie,
ed. Hausmann & Volk), 1927.
73. Bloch, B. -- Iere Conf. Internat.
Lumiere, Lausanne, 1928.
74. Eidinow, A. -- Brit. Jnl. Tuberculosis,
July, 1928.
75. Hausser, K. W. -- Strahlentherapie, 28,
1928, 25-44.
76. Schall, L. & Alius, H. J. -- Strahlentherapie,
27, 1928, 769-793.
77. Memmesheimer, A. J. -- 18th Rept. St. John's
Hosp. Derm. Soc., 1929.
78. Rohr, H. O. -- Strahlentherapie, 1929,
34, 157-189.
79. Smith, M. G. -- Amer. Jnl. Phys. Therapy,
January, 1930.
80. Bachem, A. & Reed C. I. -- Archives Phys.
Therapy, October, 1931 (Quartz Lamp, N., November, 1931).
81. Waller, M. D. -- Proc. R. Soc., B, 1931,
108, 259-263 (Quartz Lamp, S., October 1931).
Also Nos. 785 (Chap. 7);
796 886
Fluorescence.
82. Keller, P. -- Derm. Ws., April 3rd, 1926.
83. Lewin, H. -- Derm. Ws., June 19th, 1926.
84. Klovekorn, G. H. -- Derm. Zs., 1927,
50, 27-29.
85. Goodman, H. -- Amer. Jnl. Phys. Therapy,
August, 1928.
86. Woodbury, F. T. -- Phys. Therapeutics,
November, 1928.
87. Kramer, K. -- Virchow's Archiv., 1929,
274, 215-222.
88. Radley, J. A. & Grant, J. -- Fluorescence
Analysis in Ultra-violet Light (1933).
Also Nos. 131 641-650 829
Blood Effects.
89. Naswitis, K. -- Med. Klinik, 1922, No.
44.
90. Ramain, P. -- Recherches sur l'influence des
radiations solaires, ultra-violettes et infra-rouges sur le taux des globules
blancs et la formule hemoleucocytaire (Montpellire, 1923).
91. Sonne, C. -- Strahlentherapie, 1923,
16, No. 1.
92. Colebrook, Eidinow & Hill. -- British
Jnl. Experimental Pathology, 5, 1924, 54-64.
93. McCaskey, D. -- Med. Jnl. & Record,
December 17th, 1924.
94. Davis, F. A. -- Med. Jnl & Record,
August 19th, 1925 (Quartz Lamp, July, 1926).
95. Bannerman, R. G. -- Brit. Jnl. Radiology
(B. I. R.), February, 1926.
96. Gheldere, C. & Roover, M. -- C. R. Soc.
de Biologie, March 26th, 1926 (Brit. Med. Jnl., April
1926).
97. Koeppe, H. -- Strahlentherapie, 1926,
23.
98. Peemoller, F. & Franke, H. -- Strahlentherapie,
1926, 21, 165.
99. Tosi, G. -- Raggi Ultravioletti, 1926,
2, 194-213.
100. Eidinow, A. -- Lancet, November 5th,
1927.
101. Kennedy, W. P. & Thompson, W. A. R. --
Quarterly Jnl of Experimental Physiology, 1927, 18, 263-266.
102. Sanford, H. N. -- American Jnl. Dis. Children,
January, 1927.
103. Gonce, J. E. & Kassowitz, K. -- Jnl.
A.M.A., January 28th, 1928.
104. Spence, K. C. -- Brit. Jnl. Actinotherapy,
August, 1928.
105. Spence, K. C. -- Brit. Jnl. Actinotherapy,
November, 1928.
106. Eidinow, A. -- Brit. Med. Jnl., August
17th, 1929.
107. Perlman, H. H. -- Archives Phys. Therapy,
December, 1929 (Quartz Lamp, February 1930).
108. Furniss, A. -- Brit. Jnl. Actinotherapy,
December, 1930.
109. Huntemuller, O. -- Strahlentherapie,
1930, 35, 489-500.
110. Sanford, H. N. -- Archives Phys. Therapy,
March, 1930 (Quartz Lamp, May, 1930).
111. Levine, V. E. -- Archives Phys. Therapy,
July, 1931 (Quartz Lamp, September 1931).
112. Leopold, J. S. & Bernhard, A. -- Am.
Jnl. Dis. Children, April, 1932 (Quartz Lamp, N., May, 1932).
Also Nos. 595
831 848
Metabolism.
113. Rothmann, S. & Callenberg, J. -- Klin.
Ws., September 17th, 1923.
114. Pincussen, L. -- Strahlentherapie, 1924,
18, 625.
115. Steenbock, H. -- Phys. Therapeutics,
May, 1926.
116. Firth, J. B. & Russell, W. K. -- Brit.
Jnl. Actinotherapy, June, 1927.
117. Fairhall, L. T. -- Amer. Jnl. Physiology,
1928, 84, 378-385.
118. Ferri, U. -- Clinica Ped., 1928, 10,
129 (Quartz Lamp, November, 1928).
119. Lippman, A. & Volker, H. -- Klin Ws.,
January 29th, 1928 (Brit. Jnl. Actinotherapy, May, 1928).
120. Davis, S. -- Phys. Therapeutics, November,
1929.
121. Arnautov, A. & Weller, E. -- Zs. f.
d. ges. Exper. Med., May 16th, 1931 (Quartz Lamp, September
1931).
122. Brown, W. L. -- Post-graduate Med. Jnl.,
November, 1932.
123. Chick, H. -- Lancet, August 13th, 1932,
20.
Also Nos. 22
134 588 589
595
General.
124. Hausmann, W. -- Grundzuge der Lichtbiologie
und Lictpathologie (1923).
125. Hausmann, W. -- Strahlentherapie, 1923,
Suppl. 8, p. 103 (Quartz Lamp, February, 1924).
126. Eidinow, A. -- Brit. Jnl. Tuberculosis,
July, 1925.
127. Hill, L. -- Nature, May 2nd, 1925.
128. Hill, L. -- Brit. Med. Jnl., September
12th, 1925.
129. Bachem, A. -- Archives Phys. Therapy,
December, 1926.
130. Eidinow, A. -- Brit. Jnl. Radiology
(B.I.R.), January, 1926.
131. Meyer, P.S. -- Zentralbl.f.Haut Krankheiten,
22, 1926, 713-742.
132. Rost, G. A. -- The biological basis of ultra-violet
therapy (1926, 1/-).
133. Baly, E. C. C. -- Dental Surgeon, October
8th, 1927.
134. Hausmann, W. -- Die allgemeinen Grundlagen
der Lichttherapie (in Handbuch der Lichttherapie, ed. Hausmann &
Volk), 1927.
135. Kime, E. N. -- Phys. Therapeutics, December,
1927.
136. Laqueur, A. -- Lichttherapie innerer Erkrankungen
(in Handbuch der Lichttherapie, ed. Hausmann & Volk), 1927.
137. Sonne, C. -- Strahlentherapie, 28, 1928,
45-51.
138. Pincussen, W. -- Photobiologie; Grundlagen;
Ergebnisse; Ausblicke (1930, Mk.36).
139. Downes, A. -- Sunlight, Summer, 1932.
To win the patient's understanding and co-operation
it is helpful to explain briefly that actinotherapy is the therapeutic
use of rays similar to those found in sunlight, but of greater intensity;
that these ultra-violet rays have powerful bio-chemical effects, raise
the bactericidal power of the blood, and increase resistance to infection.
(See the useful notes given by Dr. L. C. Donnelly in his paper "How I use
ultra-violet energy," No. 832). A brief talk can be suited to the circumstances
of the case. Explain that little or nothing will be felt during the actual
treatment, and advise what reaction will follow. If this is expected
to be severe, prescribe suitable alleviatives (see page 40). Stay in attendance
with each patient during the earily treatments.
When actinotherapy is first administered in chronic
conditions, the first results may be reinoculation of the patient and a
temporary exacerbation of symptoms. This is frequently observed and is
usually a good prognostic sign.
Records.
Time and distance of each irradiation should be noted on the case-record card, and the resulting reaction entered at the next visit.* (*Special Record Cards for Light Treatment are supplied by the Hanovia Co. through its dealers and agents.)
Individual Treatment.
In private practice, it is most convenient to treat
the patient on a couch. If not over 20 inches high this allows the Alpine
Sun burner to be raised 40 inches from the patient. Keep the treatment
room warm (70-75 degrees F.), or use the Sollux Lamp for warming the patient.
The operator and any attendants must wear goggles; the patient should also
do so, but may be allowed to dispense with them provided the eyes are kept
shut.
Have the lamp in position by the couch before
switching on. The burner should not be directly over the patient. When
it is running at full output the patient, undressed, lies flat on the
couch and the timing clock is started. If back and front are being irradiated
2 minutes each, set the clock for four minutes and instruct the patient
when to turn over.
The skin should be quite clean, divested of grease,
powder, etc., before treatment. A hot bath or shower will both cleanse
the skin and improve its circulation, thus promoting the actinic reaction.
Loin slips are often worn during treatment; except for these, the greatest
possible area of skin should be exposed for tonic irradiation.
Collective Treatment.
In large scale clinics using the Jesionek Lamp, patients are usually treated standing or sitting. Distance of exposure is regulated by graduated circles marked on the floor, and it is a simple matter to ascertain the time for an average erythema reaction at each distance. Take individual tests to ascertain any personal idiosyncrasy, so that patients can be grouped for treatment suited to the needs of each case.
Dosage.
Several factors must be considered in correct dosage. These include:
Apparatus -- quality and intensity of radiation emitted.
Exposure, considered under:
(a) Distance (from lamp
to patient).
(b) Time of exposure.
(c) Area of skin exposed
to the rays.
Frequency of irradiaton (intervals between exposures).
The patient, with special regard to:
(a) Constitutional factors.
(b) Condition, ascertained
after diagnosis.
It is impracticable to standardize technique in terms of minutes and inches, in view of the number of variant factors. So far as any indications for exposure are given here, e.g., on the Erythema Chart (page 42), they should be understood as referring to a patient with an average skin reacton and to a Standard Alpine Sun burner (A.C. type or D.C. at 200-500 volts) of 1932 type which has been used not more than 100 hours.
Apparatus.
In this handbook, the technique of ultra-violet irradiation
is standardized on erythema reactions (see below). The practical test of
an actinic source is its power to evoke an erythema on the skin in reasonable
time. If, on test, a lamp does not fulfil this condition, it should be
renewed or replaced. For clinical work, it is essential to standardize
the map output at intervals.
The Standard Alpine Sun and Kromayer Lamps are less
powerful when set to operate on low voltage Direct Current circuits. Compared
with the higher voltage models, these lamps would require about 50 per
cent. increase in exposure. As the standard voltage in the United States
is 110, over-dosage would result from applying the time and distance factor
stated by American writers to high voltage lamps without correction.
The practitioner should, at the outset, and periodically,
standardize his own lamp by skin test, preferably on himself. This will
ensure that he is familiar with the various degrees of erythema reaction,
and repetition of the test (say, after each 100 or 200 hours of burner
use) will obviate errors due to differences in personal reactions. A simple
and practical method is as follows:
Air-cooled Lamp.
Light the lamp and allow it to burn for 10 minutes (Standard Alpine, until operatometer needle is steady). Then take a series of five exposures on the inner forearm, at a uniform distance of 10 inches from the burner. Each exposure should be made through an aperture about half-an-inch in diameter, keeping the rest of the skin covered. Convenient times are 1, 1 1/2, 2, 3, 6 minutes. On the following day observe the result, and repeat at 40 inches distance for times of 3, 5, 10 minutes. If the forearm is pigmented such tests should be made on the abdomen.
Kromayer Lamp.
Using the same method, after the lamp has burnt 5 minutes, hold the window in contact with skin of inner forearm for 10 seconds, at other spots for 25 seconds, 40 seconds and 1 minute. Next day repeat (on other arm) at 2 inches distance, for 30 seconds, 1, 2, and 5 minutes. Use a sheet of paper with cut aperture for these distance irradiations. The reactons, 1-2 days later, make it easy to standardize the erythema output of a lamp, in terms of a personal reaction. Keep a record of time, distance, and reaction, and repeat the tests when the lamp has given 100 hours operation, then after 200 hours, and so on. Thus you arrive at factors expressing the intensity of a lamp in terms of its erythema production.
Sollux Lamps.
These lamps produce no erythema and no latent reaction. Their therapeutic effect is an immediate deep-tissue hyperaemia.
Exposure.
(a) Distance. For convenience of measurement,
a distance gauge is manufactured for use with any model of the Alpine Sun
Lamp. In large clinics using the Jesionek Lamp, it is useful to fix lamp
distances by white lines permanently marked on the floor.
Whilst the mercury arc is not a point source of
radiation, the inverse square law is roughly true for the intensity of
its radiation.* (*For more accurate calculation of the dose
at varying distances, the formula: I = t/d1.6 is considered valid for the
air-cooled burner with reflector, and has been used in calculating the
table on page 35.) Note that this does not apply to the quality of
the rays; due to differential absorption by air, irradiation from a short
distance (10 inches) has a greater proportion of short-waved, counter-irritant,
bactericidal rays than from 30 to 40 inches. Sampson (786) distinguishes
between long-wave and short-wave technique on the distance basis alone.
The following reference table shows the relative
intensity of uniform time exposures given at different distances:--
| Distance
(inches). |
40 | 31 | 26 | 22 | 20 | 17 | 14 | 12 | 10 |
| Proportionate Dose. | 1 | 1 1/2 | 2 | 2 1/2 | 3 | 4 | 5+ | 7 | 9 |
Frequency of Irradiation
Intervals between treatment will vary according to the condition present and the severity of any previous skin reaction. As a general rule, do not apply repeat irradiation until the previous reacton has subsided. Authorities vary widely in their procedure for courses of light treatment, and some attempt is made below to clarify this matter by instancing typical courses of general irradiation.* (*It is appropriate to emphasize here that these times and distances are not hard and fast guides. The patient's reaction to any irradiation gives the best guidance for correct exposure at the next treatment.)
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Typical Conditions. Neurasthenia, digestive disorders, anaemia, hyperpiesis.
Book Nos. 140-159 DOSAGE
Sedative Course.
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Therapeutic Course.
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Constitutional Factors. In fixing the initial dose, the best procedure is to ascertain each patient's sensitiveness by previous tests on small areas. There are wide variations due to:-
Sex. Women require about 75 per cent. of the dosage applicable to males.
Age.Children require about half the adult dose; infants about a quarter. (Note. Infants up to 3 years old may not develop erythema reaction).
Skin. Tanned skins, dark complexions, thick fatty skins, all indicate increased dosage. Fair skins, red hair, special sensitiveness to sunlight indicate caution and a small starting dose. Albinos will probably react to a minimal dose.. Long-standing syphilis or malaria may cause violent reactions.
Weight. Some experts state that muscular and corpulent subjects show best results when irradiation is given frequently and dosage steadily increased, whilst those patients of active nervous temperament react best to smaller doses once or twice weekly only.
Body area. Different areas of the body surface
react differently to actinic rays. Bach gives a useful table of relative
sensitivity as below:
| 100 per cent. | Abdomen, chest, back, pelvis. |
| 75 per cent. | Inside forearm, outside arm. |
| 50 per cent. | Neck, face, thigh, calf. |
| 25 per cent or less. | Hands, soles of feet. |
Erythema.
The skin erythema following ultra-violet radiation develops after a latent period which may vary from one to eight hours. It is a skin flush accompanied by vascular dilation. The degrees usually distinguished are the following:
Sub-erythema.
No visible reaction, the dose being determined as
one quarter of the second degree erythema.
Synonym: "Sedative dose."
1st Degree. A reaction so slight that
it is scarcely noticed by the patient. The skin reddening is very faint,
occurs after a latent period of some hours, usually subsides within one
to two days, and is not followed by visible exfoliation. Should be administered
on the entire body, or largest possible area.
Synonyms: "Ultra-violet douche"; "Minimal erythema
dose"; "Tonic dose."
2nd Degree. A mild sunburn reaction. The reddening
is plainly visible and is followed on subsidence by slight granular exfoliation.
Subsides in about three days, leaving some pigmentation.
Synonym: "Stimulative dose."
3rd Degree. An intense reaction similar to
severe sunburn. The reddening is intense and the epidermis can be peeled
off in large strips. Takes about a week to subside, leaving pigmentation.
Essentially a local reaction.
Synonyms: "Regenerative erythema"; "Counter irritant
dose"' "Inflammatory stimulus."
4th Degree. An intense reddening, supervening
after a short latent period (about two hours) and deepening until exudation
and blistering result; persists for many days. Only administered on small
areas. Usually administered at contact, or short distance, and is thus
also a bactericidal or sterilizing dose.
Synonyms: "Dermatitis bullosa"; "Destructive dose":
"Acute inflammatory stimulus."
The erythema chart (page 42) gives data which will
assist in correlating any required degree of erythema with the exposure
factors. It should be carefully studied, but not blindly adopted as a hard
and fast rule without regard to the patient.
Demarcation.
It is simple to limit actinic reaction to any required body area, by covering the areas not to be exposed. Black paper cut to shape, plaster, etc., may be used. A very handy preparation is "Protectol" * ointment which can be used for protecting the nostrils, labia, and other areas not easily covered in other ways.
Alleviation.
Any slight irritant following an ordinary tonic dose
is easily alleviated by applying boracic or talcum powder. For more intense
erythema, cold compresses (resorcin, aluminium acetate, boric lotion, calamine
lotion, etc.) or ointment ("Hanoviol,"* 2 per cent. salicylic ointment,
zinc oxide, etc.) may be applied. Where heavy reaction has been caused
in a cavity (nostrils, etc.) a soothing suppository may be made up as below:
(*Supplied by the Hanovia Co., and Agencies.)
Al. acet. (bas. Sol.). . . . . . . . . . . . . . . . 5
Lanoline . . . . . . . . . . . . . . . . . . . . . . . 10
Vaseline alb. . . . . . . . . . . . . . . . . . . . . 20
If applied immediately after local overdose of actinic
rays, irradiation with the Sollux Lamp, using the localizer and red filter,
applied for 15-30 minutes, will obviate an undue skin reaction (see page
51).
Contra-indications.
Contra-indications for phototherapeutic treatment
include all those pathological conditions where the organism is incapable
of summoning resources to make a reparative effort under the influence
of ultra-violet rays.
This is the case with almost all the cachexias and
acute febrile diseases (congestive tuberculosis taking the first place).
Ultra-violet appears equally contra-indicated in all the cases where the
patients have to be maintained in complete repose. For example, gross renal,
hepatic, or cardiac insufficiency.
Under this heading must be included:
Conditions of auto-sensitization (scarlet fever,
small-pox, measles, pellagra, beriberi, xeroderma, hydroa aestivale, Addison's
disease.
Advanced arteriosclerosis.
Advanced heart disease with failure of compensation.
When there is any doubt whether actinotherapy should
be administered, small doses should be the rule, and careful observation
should be kept of pulse, temperature, and weight.
Photosensitization.
Certain drugs, dyes and heavy metals cause photo-catalytic
reactions when present in the system during actinic irradiation. In the
hands of experts, some of whose publications are noted (page 44), this
phenomenon has been utilized in therapeutic irradiation. Whilst photosensitization
is not yet a widely used or fully understood procedure, the practitioner
should be familiar with the commoner substances which evoke it, as cautious
dosage of actinic rays is indicated when these are being administered:
Drugs. Quinine, trypaflavin, eosine, chlorophyll,
pyridine, gonacrine, methylene blue, and the other fluorescent dyes.
Endocrines. Insulin, adrenalin, pituitrin,
thyroid.
Metals. Heavy metals circulating in the blood
increase the effect of ultra-violet rays. Again, the effects of drug therapy
in which these metals are administered are distinctly increased under the
influence of the rays. This applies to mercury, iron, bismuth, gold, silver,
etc., and especially to calcium and its salts.
Desensitizers. It is stated that ingestion
of the following substances retards actinic reactions:
Resorcin (3 grains, taken
one day before irradiation).
Camphor and its derivatives.
|
|
|
|
|
|||||||
|
|
|
|
||||||||
|
|
|
|
|
|
|
|
|
|||
| Sub-Erythema. | No visible reaction. | "Sedative Dose." May be repeated daily on entire skin area. | Usually taken as 1/4 of the 2nd degree erythema dose, ascertained by test. |
|
|
|
|
|
||
| First. | Very slight; causes no subjective symptoms. Reddening of skin scarcely visible and disappears within 24 hours. | "Tonic Dose." May be administered on entire body and repeated daily, or every second day. |
|
|
|
|
|
|
|
|
| Second. | Symptoms of mild sunburn. Reddening is visible and followed by granular exfoliation. | "Counter Irritant Dose." Two-three day intervals before repetition. |
|
|
|
|
|
|
|
|
| Third. | Symptoms of severe sunburn. Reddening intense. Skin will peel off in large strips. | "Simulant" or "Desquamation Dose." Usually administered on limited area only. Allow 4-7 days interval. |
|
|
|
|
|
|
|
|
| Fourth. | Very intense reddening with oedema and formation of blisters in the epidermal layers. | "Bacterial Dose." Gives protein-shock reaction. Given on limited focus only. Repeated as required. |
|
|
|
|
|
|
|
|
| Note. For D.C. 110 v. model add 50% to above exposures. Halve the above exposure for infants. | Note. When the blue filter is used, allow 4 x above exposures. With rod applicators allow 2 x above exposures on skin, 3 x on normal mucous membrane. | |||||||||
REFERENCES TO LITERATURE.
Dosage.
140. Mayer, E. -- Amer. Rev. Tuberculosis,
October, 1922.
141. Dahlfeld, C. -- Strahlentherapie, 1923,
16, 75-95.
142. Keller, P. -- Strahlentherapie, 1923,
16, 1924, 17.
143. Jesionek, A. & Rothmann, S. -- (In irrtumer
der allgemeinen Diagnostik und Therapie, No. 4, 1924).
144. Donnelly, L. C. -- Jnl. Radiology, May,
1925.
145. Eidinow, A. -- Lancet, August 15th,
1925.
146. Hill, L. & Eidinow, A. -- Practitioner,
August, 1925.
147. Eidinow, A. -- Lancet, September 25th,
1925.
148. Thedering, F. -- Brit. Jnl. Actinotherapy,
November, 1927.
149. Thedering, F. -- Strahlentherapie, 1928,
28, 602-610.
150. Kovacs, Anderson, Bridge, et al. -- Med.
Jnl. & Record, December 4th, 1929.
151. Furniss, A. -- Brit. Jnl. Actinotherapy,
June, 1930.
152. Blumenthal, Keller, Lomholt, et al. -- Derm.
Ws., September 5th, 1931.
Also Nos. 744 786 790 791
793 796 799 852
Contra-indications
152a. Dufestel, L. G., et al. -- Brit. Jnl. Actinotherapy,
April, 1928
152b. Hickel, R. -- Reactions, incidents, accidents,
provoques par les rayons ultra-violets (1932. 15 frcs).
Photosensitization.
153. Ostermann, M. -- Brit. Jnl. Actinotherapy,
September, 1926.
154. Courmelles, F. -- Phys. Therapeutics,
February, 1928.
155. Jausion, H. -- ler Conf. Int. de la Lumiere,
Lausanne, 1928.
156. Lassen, H. C. A. -- Strahlentherapie,
1928, 27, 757-768.
157. Hindley-Smith, J. D. -- Brit. Jnl. Actinotherapy,
April, 1929.
158. Woodbury, F. T. -- Phys. Therapeutics,
December, 1929.
159. Eidinow, A. -- Brit. Jnl. Radiology,
March, 1930.
Also No. 132 152b 789 (Chap.
13); 796 797 831 898
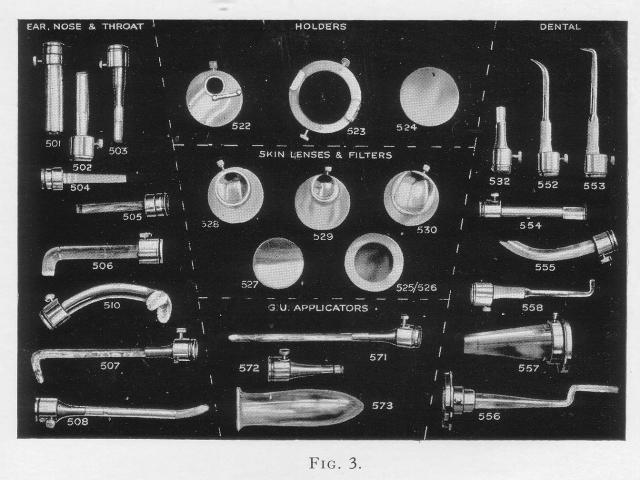
APPLICATORS FOR THE KROMAYER LAMPS
As a guide in selecting applicators, the standard forms in use are illustrated and briefly described below:
No.
| *501 Round rod, 17 x 80 mm.
*502 Round rod, 12 x 80 mm. |
(These are of general utility, e.g., for treating nodules, small ulcers, gingiva, conjunctiva, etc. |
| *503 Round rod, 5 x 80 mm. | For the auditory canal. |
| 504 Wedge (adults) 10 x 80 mm.
505 Wedge (children) 8 x 74 mm. |
Designed for nasal irradiation. These applicators have a centimetre scale etched on the quartz to assist in regulating exposure. Also useful for irradiating a narrow sinus. |
| *506 Curved rod, 11 x 110 mm. | Laryngoscope, designed by Dr. Sampson for laryngeal tuberculosis. Also
used in dental surgery for gingival irrradiation on lingual aspects.
|
| 507 Hooked rod (spatulate tip) 8 x 150 mm. | Introduced by mouth for irradiation of naso-pharynx. |
| 508 Rod (flattened at tip) 6 x 140 mm. | For irradiation of nostrils and posterior nares; deep sinus work, etc. |
| *510 Rod (with forked end) | Dr. Hindley-Smith's special tonsil applicator. |
| 522 Socket disc. | This (with No. 523) is essential for fixing any applicator to the Kromayer Lamps. It embodies a three-way lever giving white (unfiltered) light, blue light, or cut-off, as required. |
| 523 Holder. | For the Standard Kromayer Lamp, used with No. 522 for attachment of any rod applicator. |
| 523a. Holder | For the Kromayer Lamp (Model II). Similar to No. 523. |
| 524. Lens cover (metal). | For Kromayer Lamp . Safety screen for use when lamp is lit, but not being applied. |
| 581. Lens cover (mica in metal frame). | For Kromayer Lamp (Model II). Serves same use as No. 524. |
| 525. Uviol blue window (in metal frame). | For Standard Kromayer Lamp. Applied in front of the lamp window. Cuts off the shorter ultra-violet rays (below 2800 A.U.) giving a milder radiation with deep penetration. Necessitates about four times the exposure of unfiltered radiation. (See pages 14-46). |
| 525a. Blue window (in metal frame). | For Kromayer Lamp (Model II). Same purpose as No. 525. |
| 526. Diagnosis filter (in metal frame). | For Standard Kromayer Lamp. Applied in front of the lamp window. This filter serves for fluorescence -- diagnosis of skin infections, e.g., ringworm. (See pages 14-142). |
| 526a. Diagnosis filter (in metal frame). | For Kromayer Lamp (Model II). Same use as No. 526. |
| ^527. Crystal quartz window. | (Spare part for the Standard Kromayer Lamp). To be inserted with the bevel edge outward. |
| ^528. Medium Skin Lens, 28 mm. 0 | Used in compression treatment for dehaematization and deep penetration. |
| ^529. Small Skin Lens. 20 mm. 0 | Used in compression treatment for dehaematization and deep penetration. |
| ^530. Large Skin Lens, 30 x 34 mm. | Used in compression treatment for dehaematization and deep penetration. |
| 532. Round rod, 8 x 50 mm. | For gingival work. |
| *552. Round rod with half bend, 5 x 100 mm., tapered | Pyorrhoea applicators, for penetration of pus pockets. Also valuable in ophthalmic work to irradiate conjunctival fornices, small ulcers, etc. |
| *553. Round rod with right angle bend, 5 x 100 mm. tapered tip. | Pyorrhoea applicators, for penetration of pus pockets. Also valuable in ophthalmic work to irradiate conjunctival fornices, small ulcers, etc. |
| *554. Round rod, 12 x 100 mm. | For facial aspects of gingiva and irradiation of small foci elsewhere. |
| *555. Curved rod, 12 x 120 mm. | For lingual aspects of gingiva and other oral lesions. |
| 556. Bayonet rod, 6 x 170 mm. | Designed by Dr. Zilz for irradiating oral lesions of difficult access. |
| ^557. Conical oral applicator, 100 mm. long, tapering to 15 mm. 0 | This applicator gives heavy concentration of the rays on a small area, ensuring heavy reaction with short exposure. |
| *558. Right angle rod with bulbous tip, 8 x 110 mm. | Primarily for irradiation of tooth sockets after extraction. |
| 571. Rod, olive shaped tip, 6 x 170 mm. | A long rod for urethral irradiation, also valuable for empyema and deep fistulae. |
| 572. Rod, 5 x 70 mm. | A general utility rod applicator. |
| 573. Quartz speculum, small, 32 x 112 mm. | For vaginal irradiation. The speculum is placed in the patient first and lamp brought up. A rod applicator affixed to the lamp can be used within the speculum to irradiate small ulcers, etc. The small speculum is also used for rectal irradiation in a similar way. |
| 574. Quartz speculum, medium, 32 x 118 mm. | For vaginal irradiation. The speculum is placed in the patient first and lamp brought up. A rod applicator affixed to the lamp can be used within the speculum to irradiate small ulcers, etc. The small speculum is also used for rectal irradiation in a similar way. |
| 575. Quartz speculum, large, 38 x 112 mm. | For vaginal irradiation. The speculum is placed in the patient first and lamp brought up. A rod applicator affixed to the lamp can be used within the speculum to irradiate small ulcers, etc. The small speculum is also used for rectal irradiation in a similar way. |
^These applicators are ground from crystal quartz,
and must be sterilized cold with alcohol, etc. All other applicators are
of fused quartz and may safely be sterilized by boiling. Remember that
the ultra-violet rays are themselves powerful bactericidal agents and will
quickly destroy any germs on the window or rods.
| Fig 3. APPLICATORS
FOR THE KROMAYER LAMPS
The technique of irradiating the membranes
which line orifices of the body necessitates applicators of suitable design.
The forms here illustrated are, in nearly every case, designed by specialists
in the various branches of medical work under which they are classified.
Details of dimensions and uses are stated opposite.
|
Local Irradiation.
1. Kromayer Lamp.
It should be remembered that local irradiation with
the Kromayer Lamps is a different procedure to treating a small area with
the air-cooled models. The shorter ultra-violet rays, which have most powerful
bactericidal properties, are readily absorbed by air. With the Kromayer
Lamps, the radiation penetrates only 1/2 inch of water. This filters out
the infra-red rays, but transmits the ultra-violet rays above 2000 A.U.
practically unweakened.* Application of window or rod in contact means
utilizing these short bactericidal rays in full intensity. (*
The diagram on page 18 shows the output of the Kromayer Lamp.)
In distant irradiation, the Standard and Model II
Kromayer Lamps should usually be applied about 2 inches from the skin surface,
at right angles. If well defined, the lesion may be demarcated by plaster,
or black paper cut to shape and applied to the skin. Remember that in treating
ulcers, erysipelas, etc., it is essential to include a margin of healthy
skin when giving treatment.
2. Alpine Sun Lamp.
To produce a second or third degree erythema on the
scalp, face, a limb, etc., it is usually sufficient to cover the unexposed
areas and bring the Alpine hood to correct distance. Remember that the
rays should always be directed at right angles to the treatment surface.
Lesions which are quite small, and where heavy reactions
are not indicated, may be radiated through the aperture in the Alpine Sun
lower hood. Do not apply the Alpine Sun at less than 8 inches burner-to-skin
distance.
Compression irradiation.
Ultra-violet rays are absorbed in the capillary blood
vessels. When the skin is dehaematized by compression, the rays penetrate
into the deeper epithelial layers.
The quartz window of the Standard Kromayer Lamp
may itself be applied directly to the skin in compression treatment. More
effective dehaematization is secured by compression through one of the
skin lenses (Nos. 528-530).
Deepest penetration is obtained by using the blue
filter in contact with the Kromayer Lamp window, and giving about four
times the normal unfiltered light exposure to produce an equal degree of
erythema.
Where a long exposure under compression is given,
it is sometimes found convenient to bind the lamp burner firmly into position.
When using this procedure with the Standard Kromayer Lamp, take care that
the burner is maintained in correct position throughout treatment.
The lamp front can be sterilized after use by washing
with sublimate solution.
Treatment with applicators.
A quartz rod transmitting ultra-violet rays acts
as a lens throughout its length. Practically the same quality and intensity
of radiation which enters from the burner is emitted at the treatment end.
The quartz rod obviates the losses in intensity and quality caused by air-transmission;
still more, it allows the beam to be deflected so that irradiation can
be applied to foci (larynx, etc.) which are inaccessible to direct irradiation.
The successful use of the Kromayer Lamp depends
largely on due employment of the applicators. Their various uses are described
briefly below:
Skin Treatment
Normal mucous membrane will tolerate about 50 per
cent. greater exposure than the skin of the abdomen, but great variations
occur due to pathological changes. For example, the nasal membrane may
require only 30 seconds exposure in cases of hay fever, but 10 to 15 minutes
for ozaena.
When producing a heavy reaction in a cavity, measures
should be taken to prevent blistering the skin (nostrils, labia, etc.)
at its entrance. A practical way is to insert the applicator alone to the
full length required, then grease the outside skin with "Potectol" or lanoline.
Do not apply the grease first, or it will adhere to the applicator and
interfere with treatment. After this is done, bring the Kromayer burner,
ready lit and running at correct intensity, into position and affix to
the applicator.
The notes given under the various conditions in
this handbook, combined with the descriptions of applicators following,
will enable the practitioner to select applicators suitable for treating
all indications.
Sinus irradiation.
A deep, irregular sinus, fistula, or septic wound, may be irradiated by flooding the cavity with one of the photo-sensitive dyes and irradiating with the Kromayer Lamp and a suitable applicator (e.g., No. 571) dipping into the solution. The aniline dyes, eosine, acriflavine, gentian violet, fluorescein, in 1/1000 water or glycerine solution, are usually employed, or mercurochrome in suitable cases. Donnelly states that gentian violet has special affinity for staphylococci, streptococci, and anthrax; and acriflavine for gonococci, the colon and dysentery groups.
References:
159a. Kromayer, E. -- Derm. Zs., 66, 1933, 79-84
(Quartz Lamp, S, July 1933).
Also Nos. 837 913
On a strict definition, "actinotherapy" means the
medical application of short, actinic, ultra-violet rays, and indicates
the use of "cold" actinic sources such as the quartz lamp. Its meaning
is, however, extended to include all forms of light treatment.
At the other end of the visible spectrum are the
luminous heat and infra-red rays, generated by the sollux Lamps. This group
of radiations form a valuable complement to the ultra-violet rays. They
have greater power of tissue penetration, and take immediate action. These
"thermal" rays do not produce the powerful secondary physiological reactions
characteristic of the photo-chemical "actinic" rays; their effect is a
deep penetrating hyperaemia of long duration. Locally, they produce a blood
temperature exceeding the highest known fever, with consequent increase
in the processes of oxidation and immunization (phagocytosis). This points
to the indications for their therapeutic use in acute conditions associated
with inflammaton and pain.
Some conditions exhibit the best response under
combined irradiation, in which both the actinic and thermal rays are utilized
to reproduce the full range of sunlight. Frequently the heat rays are subsidiary:
they serve only to warm the unclothed patient, to improve skin-circulation,
and so prepare the way for a satisfactory actinic reaction. In certain
conditions (e.g., rheumatism, neuritis) their action is essential to relieve
the acute symptoms, whilst the subsequent actinic reaction assists to rebuild
tone and promote recovery.
The Sollux Lamp generates, in addition to invisible
infra-red, a proportion of visible red and yellow radiation. Its output
characteristics are reproduced on the special graph (page 18) with which
is correlated a graph of the comparative tissue-penetrating power of different
wave-lengths. Red light, and the shorter infra-red rays, are the most penetrative
of all wave-lengths employed in light therapy; comparison of these graphs
makes this evident. The longer-waved infra-red do not reach the underlying
tissues, and tend to overheat the skin when applied in excess (177).
The red filter with the Sollux Lamp produces a radiation
with the maximum of deep penetrating rays in proportion to the other radiations
present.
Technique.
The reaction to these rays is visible during treatment in the form of hyperaemia; the irradiated area is deeply suffused with blood. Note that deep tissue hyperaemia reaction is the aim in most instances, and in producing this, precautions may be necesssary to prevent superficial burns. These are obvious; e.g., greasing the skin before the first treatment; cooling the skin by an electric fan during irradiation, etc.
Local Irradiation.
Either the Standard Model (1000-watt bulb) with localizer
fitted, or the small model (300-watt bulb) may be used. The technique is
similar for both lamps, but the Standard Lamp will naturally produce speedier
results.
When using the Standard Lamp for local treatment,
do not switch on full intensity. Move the resistance setting back to stud
4 or stud 3, otherwise internal overheating may destroy the bulb. Never
cover the lamp with draperies.
Place the patient in a comfortable position, preferably
reclining, and adjust the lamp so that the rays are concentrated on the
focus of the inflammation to be treated. With the Standard Lamp, attach
the localizer.
The distance of skin from the cork ring of the reflector
should be as short as the patient can tolerate without discomfort. In practice
this is found to be about 6 inches for the first treatment, which can be
reduced to 3 or 4 inches at subsequent sessions. Delicate skins (e.g.,
young children, blonde females) may necessitate precautions as outlined
above to prevent superficial burns.
To produce the required deep tissue hyperaemia,
prolonged irradiation is essential. The first treatment should be not less
than 20 minutes, and local irradiation may safely be prolonged up to an
hour at each session. Local treatment may be repeated daily, or twice daily,
or even more frequently in acute conditions.
Precautions.
When irradiating the face, the eyes should be protected by the use of cloth pads, or special goggles proof against infra-red rays. The patient should avoid exposure to cold or draughts soon after treatment.
General Irradiation.
Use the 1000-watt Model Lamp. If a special region
requires treatment (e.g., the thorax in pleurisy or pneumonia) demarcate
by clothing, etc. Distance should be the shortest possible consistent with
uniform irradiation over area. Maximum time 60 minutes each session.
In giving combined heat and ultra-violet therapy,
always administer luminous heat before or during the actinic radiation.
The eyes should be shielded from the rays.
The Colour Filters.
Red light is stated to be "antagonistic" to
ultra-violet rays in its therapeutic action. Thus a local overdosage of
quartz light can be counteracted by local irradiation for at least half-an-hour
with red light; this will obviate the blistering and severe pigmentation
which would otherwise follow:
The therapeutic indications for red light are:
(1) After-treatment of local,
actinic overdosage. In such conditions as seborrhoea and acne where it
is necessary to bring about severe reactions with the quartz lamp, after-treatment
with red light will effect quicker restoration of healthy skin and obviate
severe pigmentation (164 173).
(2) For drying up acute weeping forms of eczema
(795).
(3) For the treatment of pustular eruptions on the
skin; in such cases healing takes place without scars.
Blue light, used for prolonged local irradiation,
is stated to cause local anaemia. It has been used:--
(1) For pre-operative treatment, to cause local
anaesthesia (assisting cocaine, etc.)
(2) As an anodyne in articular and traumatic extravasations.
(3) For treating trigeminal neuralgia and acute
coryza.
The Daylight Filter has no therapeutic value, but is useful in dental and surgical practice for diagnosis and other purposes which necessitate a colour-true light.
REFERENCES TO LITERATURE
160. Cemach, A. -- Monats. f. Ohrenheilk.,
1922, 56, No. 7
161. Sonne, K. -- Strahlentherapie, 1925,
20, No. 1, and Phys. Therapeutics, April 1926.
162. Benoist, C. -- Amer. Jnl. Phys. Therapy,
October, 1926, and Brit. Jnl. Actinotherapy, September, 1926.
163. Levick, G.M. -- Brit. Jnl. of Rad., May 1926.
164. Guillaume -- Bull & Memoires de la Soc.
Med. des Hospitaux de Paris, 1926.
165. Kraft, F. de., et al. -- Phys. Therapeutics,
April, 1927.
166. Gill, A. B. -- Jnl. Amer. Med. Assn., October
8th, 1927.
167. Kellog, J. H. -- Phys. Therapeutics, October
1927.,
168. Heusner, H. -- Therapeutische Monats.,
1928, No. 6.
169. Johnson, W. T. -- Phys. Therapeutics, January,
1928.
170. Goodman, H. -- The Physics and Physiology of
infra-red radiation (Heat), 1929.
171. Kellog, J. H. -- Brit. Jnl. Actinotherapy,
March 1929.
172. Sonne, K. -- Archives Phys. Therapy, March,
1929.
173. Shattock, F. M. & Waller, M. -- Lancet,
November 2nd, 1929.
174. Brown, R. K. -- Brit. Jnl. Actinotherapy,
April, 1930.
175. Troup, W. A. -- Therapeutic Uses of infra-red
rays (1930).
176. Halla, F. v. -- Deutsche Aerzte-Zeitung,
March, 1931, No. 253 (Quartz Lamp, S., January, 1932).
177. Hill, L. -- Brit. Jnl. Phys. Med., September,
1931.
178. Libbert, E. L. -- Amer. Med.,April,
1932 (Quartz Lamp, N., July, 1932).
{kind=link}
{kind=link}
{kind=link}